unicorn
-
Posts
2,701 -
Joined
-
Last visited
-
Days Won
6
Content Type
Profiles
Forums
Events
Everything posted by unicorn
-
 I don't understand your posting. I go to musicals to enjoy the singing and dancing, not because I intend to jack off in the theater while focusing on one of the cast members. And I gladly paid $200 for my two tickets, not worrying about the $5.50 per gallon we're paying over here in California, thanks to Donny Dementia. However, when I do see an handsome actor, I do search Google Images to see if there are shirtless pix I can use to J/O. There are a lot of "actors/models" here in LA. Which reminds me of that delightful soft-core porn movie:
I don't understand your posting. I go to musicals to enjoy the singing and dancing, not because I intend to jack off in the theater while focusing on one of the cast members. And I gladly paid $200 for my two tickets, not worrying about the $5.50 per gallon we're paying over here in California, thanks to Donny Dementia. However, when I do see an handsome actor, I do search Google Images to see if there are shirtless pix I can use to J/O. There are a lot of "actors/models" here in LA. Which reminds me of that delightful soft-core porn movie: -
Looks as though he's quite limber, too! 😍

-
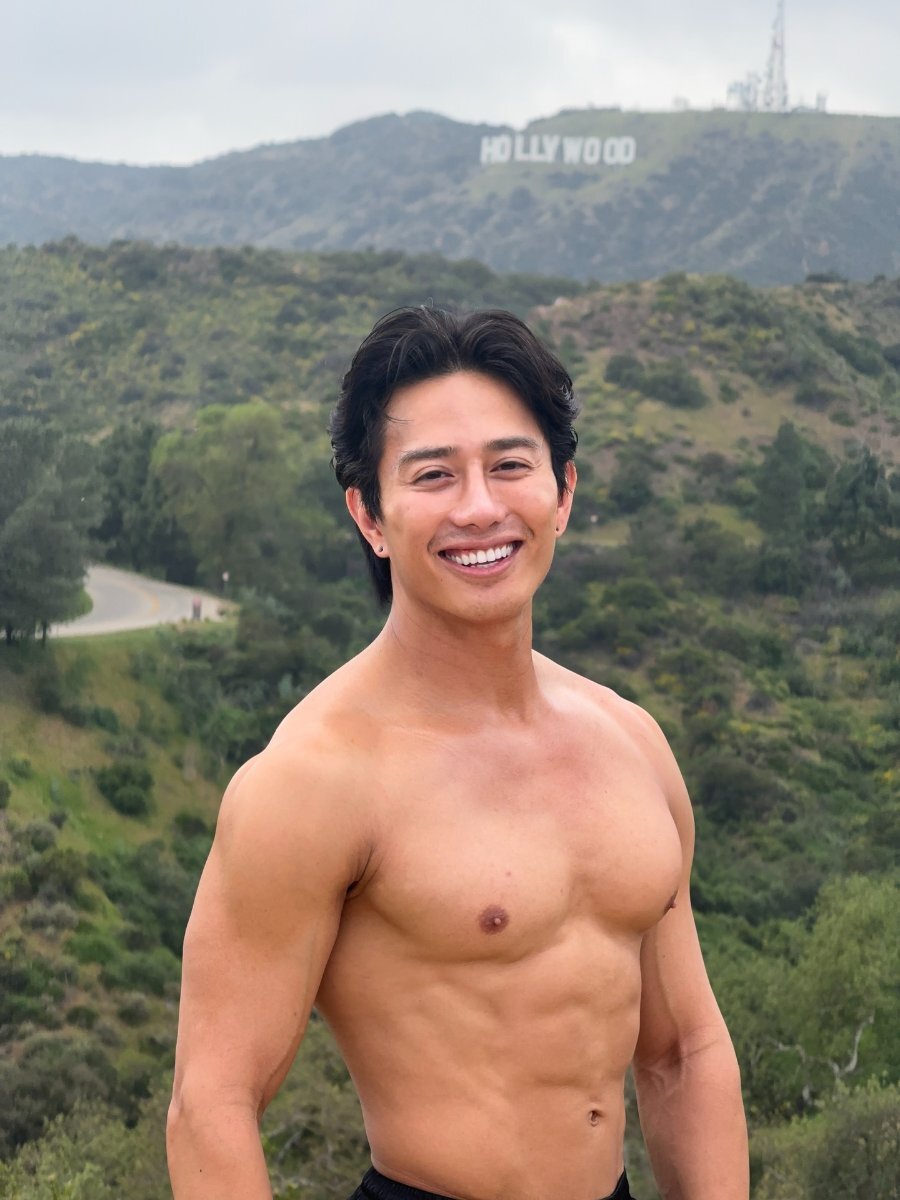
I was looking up a show recommended by an email of a musical I like, Flower Drum Song. In looking up the cast, one cast member immediately caught my eye: Joven Calloway, a member of Actors' Equity Association. I looked him up on Google Images to see if he had at least shirtless photo to which I could jack off. Boy, did I hit the jackpot! Not only does his Facebook account have lots of shirtless pictures, but it also includes links to multiple adult websites such as OF, JFF, and Sean Cody! In all of my horny years of looking up cast members in mainstream shows, I can't recall getting such a treasure trove! Do you every look up cast members for shirtless photos? Have you ever been surprised to discover a porn career in addition to a mainstream career? https://www.eastwestplayers.org/flower https://www.facebook.com/jkabobs/ https://linktr.ee/Jkabethandale https://www.famousbirthdays.com/people/joven-calloway.html



-
Also reminds me of a local (Los Angeles) story in which the Los Angeles Times found out that people were being paid to make false sex abuse accusations against the county of Los Angeles for cash: https://www.latimes.com/california/story/2025-10-16/sex-abuse-fraud-claims-la-county-victims "...Austin Beagle, 31, and Nevada Barker, 30, said they were trying to sign up for food stamps this spring when someone offered them a background role outside a county social services office in Long Beach. They thought the gig seemed intriguing, albeit a bit unusual. The offer came not from a casting director, but a man hawking free cellphones. The filming location was, oddly enough, a law firm in downtown Los Angeles. Maybe this was how actors were recruited here, they figured. The couple had recently moved from the remote ranching town of Stinnett in the Texas panhandle, and the recruiter seemed to appreciate their Southern drawl. They hopped on a bus, excited to make $200 between them. “They said we’d be extras,” said Beagle, who was unemployed at the time. “But when we got to the office, that’s not what it was at all.” The couple said they arrived at the lobby of Downtown LA Law Group. A Times investigation published earlier this month found seven plaintiffs represented by the firm who claimed they received cash from recruiters to sue the county over sex abuse, which could violate state law. Two said they had never been abused and were told to manufacture their claims...".
-
Found the ideal entertainment for my birthday party
unicorn replied to forrestreid's topic in The Beer Bar
https://www.guinnessworldrecords.com/news/2021/6/minnesota-teen-reclaims-record-for-largest-mouth-gape-664425 -
Sergio Fernandez: https://www.facebook.com/reel/1468677708199535
-
Found the ideal entertainment for my birthday party
unicorn replied to forrestreid's topic in The Beer Bar
You realize he's not gay, and lives in Northern Ireland? -
The point is that you simply choose to believe the alleged victims (in fact, you label them "victims" rather than "alleged victims," totally discounting any possibility you might be wrong). The human tendency to believe victims should be tempered by a willingness to examine facts, and not just statements. Currently, there is zero supporting hard evidence. One would be hard-pressed to even estimate the chance that these accusations are true (or false). At least if they were to test the out-of-wedlock children's DNA, they could show that the odds aren't zero that Huerta is being truthful. Of course, this wouldn't show whether or not the sex was consensual--just that sex between the two did happen. The fact of the matter is that neither you nor I know whether these allegations are truthful. Is she just trying to cast herself as a victim? Trying to improve her reputation after giving up two out-of-wedlock children for adoption? One piece of fact that makes me a bit uneasy at taking the accuser at face value is the fact that she claims two episodes of unwanted sexual intercourse (though in one case she says she was "manipulated" into consenting), and became pregnant each time. Even if Chavez was extremely unlucky, and happened to time the sex (both times) during the 1-2 days before ovulation, there's still only a 10-30% chance of pregnancy resulting in a live birth each time: AI Overview The probability of pregnancy from a single act of unprotected intercourse with a fertile woman varies significantly based on timing, ranging from nearly 0% outside the fertile window to approximately 10-30% during the most fertile days (1–2 days before ovulation). On average, the likelihood is about 3-4% per act of intercourse over a full cycle. The New England Journal of Medicine https://www.nejm.org/doi/full/10.1056/NEJM199512073332301 So even if we give the most generous interpretation of the data, that he happened both times to have sex with her during her two fertile days per cycle, and that the odds are 30%, not 10%, that still gives the odds of becoming pregnant both times to be 30% X 30%, or 9%. Outside the peak two days, or if we take the middle range of estimates, the odds drop dramatically. 9% is simply the maximum odds, with the most generous interpretation of the data, of two episodes of sexual intercourse during the fertile window resulting in live births. (I should also note that Huerta was in her 30s both times, hardly a woman's most fertile years) Even if the out-of-wedlock children are shown to be Chavez's, these data would make one have to consider the likelihood that his two children are more likely to have resulted from multiple (presumably consensual) sexual acts, rather than from two unwanted ones. There is little disincentive to falsely accuse, as prosecutions against those who falsely accuse are rare. In Huerta's case, the odds are zero, since she didn't make these accusations under oath, so could not be prosecuted for perjury. This article describes a rare case in which the false accuser was prosecuted: https://www.prosecutorintegrity.org/pr/99-of-false-accusations-go-unpunished-center-for-prosecutor-integrity-asks-why/ "99% of False Accusations Go Unpunished.... Nikki Yovino of New York falsely accused two football players at Sacred Heart University of rape. The woman later admitted that she had lied to gain the sympathy of a prospective boyfriend. As a result, Yovino was sentenced to one year in prison, plus two years of probation... One of the falsely accused men, Malik St. Hilaire, sadly recounted, “I went from being a college student, to sitting at home being expelled, with no way to clear my name. I just hope she knows what she has done to me. My life will never be the same. I did nothing wrong, but everything has been altered because of this.”...False allegations are widespread in the United States. A national survey sponsored by the Center for Prosecutor Integrity found that 8% of Americans — 11% of men and 6% of women — report being falsely accused of sexual assault, domestic violence, or child abuse. The 8% figure represents 20.4 million adults (2)...".
-
Obviously, neither you nor I has enough (nor will we ever have enough) information to believe or disbelieve the accuser. It's certainly problematic when one has the mindset that the accused has to "disprove" allegations in order to be considered possibly innocent, especially among those whose minds is already set. That's the definition of mob mentality (and many have been lynched because of it). How would you like it if you were accused of a crime, and told no one would believe you unless you could "disprove" the allegations? I guess that still happens in some countries--one would hope not advanced societies. Accusers get plenty of sympathy, not grief, especially from those close to them. It also wouldn't surprise me if Cesar Chavez day were renamed Dolores Huerta Day. At this point, one is deluding oneself if one thinks one knows the truth. It's really unknowable at this time. One can only wonder: why bring up these accusations now? If it were true that bringing up the accusations results only in "grief," there would be no motive. No one is accusing her of lying. There's no way to tell either way. There have certainly been examples of false accusations, including the blatant lies discovered in the Duke Lacrosse players' case, which ruined innocent men's lives. While not as clear-cut, the Kobe Bryant case was probably another such case. I can only wonder why Huerta is bringing this up over six decades later, and over three decades after Chavez's death. I find the overnight rush to take down his statues and murals troubling.
-
Is an actor speaking in another accent betraying himself?
unicorn replied to unicorn's topic in The Beer Bar
I, too, am confused by some posters' comments. In looking it up, Google tells me: "Meryl Streep portrayed Margaret Thatcher, the first female Prime Minister of the United Kingdom, in the 2011 biographical drama film The Iron Lady. Streep won the Academy Award for Best Actress for this performance, which explored Thatcher's rise to power and her later years." -
Yup. People magazine was just trying to make her sound like a whiner.
-
At this point, obviously there's no way to really know. Even if it happened, what's the point of bringing it up now, decades after he died? It's one thing to bring these matters up promptly, so the perpetrator can be apprehended and prevented from repeating noxious behavior. What can the accusations accomplish at this point--other than tarnish his reputation?
-
Dolores Huerta, a 96 year-old labor activist who worked with the more famous labor activist César Chavez, has waited until 33 years after his death to accuse the decedent of raping her 60 years ago. Supposedly, one of the incidents (1966) was forcible rape in the back of Chavez's car. She also described an earlier encounter in August 1960 in which "she felt pressured to have sex with him in a hotel room during a work trip in San Juan Capistrano". Apparently both of these trysts resulted in childbirth, and both were adopted and not made aware of the alleged circumstances of their conception until now. Almost overnight, municipalities and other organizations have removed artwork made to commemorate Chavez. No one has waited to even test the two to find out whether the accusation of unwanted sexual activity is even plausible. Of course, we'll never hear Chavez's version. I have to wonder why Huerta is bringing this up now? Does she want César Chavez Day to be renamed Dolores Huerta Day? (I can see that happening) I guess I shouldn't be surprised at how quickly people can rush to judgment--a kind of mob mentality. https://apnews.com/article/latino-leaders-speak-out-about-chavez-allegations-f1b24d3c6bdf71b326b63d51f80ea957 Memorial in Fresno being covered up: Statue in San Fernando being removed. It seems it was important to cover it up before being removed: Mural being covered in Santa Ana: Statue being removed in Denver: All of these accusations made decades after a person's death feel rather unseemly to me. I also find the rush to judgment disturbing.
-
He looks like a wax figure to me. Too much plastic surgery? https://sbsstar.net/article/N1008074800/just-b-bain-becomes-the-first-kpop-boy-group-member-to-come-out#1
-
-
Yeah, I suppose you're right. She does sound more tongue-in-cheek than complaining.
-
There's this extremely handsome 36 year-old actor I follow on social media, Jason Caceres, who recently put out a blurb on Facebook. In the blurb, he describes firing his manager when she suggested he take "accent reduction" lessons to get the "gay" out of his voice, so that he could have more acting opportunities. His speech must be described as very gay, one must admit. That being said, the last movie I saw, Crime 101, starred Chris Hemsworth, an Australian, and Barry Keoghan, an Irishman. They play American characters, so they've obviously been trained not to speak with Aussie or Irish accents. I doubt they're ashamed of the way they normally speak, but rather realize that a good actor needs to be versatile. I think it's actually a feather in the cap for them that they can play American characters better (at least according to the casting director) than any American can. There are a lot of successful gay actors, and the best of them can play both straight and gay characters (i.e. Matt Bomer, Neil Patrick Harris, Zach Quinto, etc.). While Jason Caceres certainly has nothing of which to be ashamed, I suspect he could get a lot more acting gigs if he could play a wider variety of parts. Yet all of the comments on his clip on Facebook applaud his firing of his manager. Do you think he's being wise? https://www.facebook.com/reel/1622663045969088


-
Well, I can understand the situation with Frank more than with Fred. After all, Frank lives across the continent, so there isn't much opportunity for friendship. I suppose it would be a gift to let Frank know how his behavior affects others (I suspect Frank's neurodivergent), but I can see why my husband wouldn't bother. Fred has had a somewhat unusual life, and I would have liked to get to know him better. He seems like a decent person, perhaps overly attention-seeking?
-
Jane Fonda apparently complained that it was Barbara Streisand rather than herself who eulogized the late Robert Redford. In poor taste? https://people.com/jane-fonda-says-barbra-streisand-didn-t-deserve-to-do-robert-redford-oscars-tribute-she-did-1-movie-i-did-4-11927207?campaign=17305911&did=22530450-20260316&hid=089247988732f9a900151e1f8c73f2c531df3c3a&lctg=089247988732f9a900151e1f8c73f2c531df3c3a&lr_input=3911d0b923e8d92c50f8b74007080afa59d66697825b8a1e414be8db883b8062&tag=latestcatalog_ppl_comments "Jane Fonda is wishing she could have paid tribute to her dear, departed friend Robert Redford. At the 98th annual Academy Awards on Sunday, Barbra Streisand took the stage as part of the ceremony’s In Memoriam segment to honor Redford, who died on Sept. 16, 2025 at age 89. “I want to know how come Streisand was up there doing that for Redford?” Fonda, 88, quipped to Entertainment Tonight at an Oscar night party. She playfully added that Streisand, 83, “only made one movie with him, I made four! I have more to say.”...".
-
In December, my husband connected with a handsome young senior financial executive with the cruise company, "Frank," while we were on a cruise in Antarctica. We socialized a bit together while on the cruise, and mentioned that we were going to go on a cruise with a sister cruise company (within his company's umbrella) in February. My husband said that we'd keep in touch and try to meet in Miami before our next cruise left (he lives/works in Miami, and the cruise was leaving from Miami). A week or so before we were going to leave, I asked him if he'd arranged a meeting for Frank and us, and he said that he ghosted him. Apparently, they were texting each other, and Frank texted "I know about West Hollywood gays, LIKE YOU," and also asked "So what are YOU doing up at this hour?" (it was 3:30 AM on a Monday, and he was up for whatever reason; I can only assume Frank was getting ready to go to work?). So that was the last text. In the meantime, I met an interesting internet personality at a Christmas party, whom I'll call "Fred." Neither of us finds him at all attractive, but I find his life story interesting, so I asked if I could invite him over for some drinks in January. We had drinks at our place, and got to know him better. Since I was so interested in his story, I did pepper him with questions. I felt I got to know him better, and I asked my husband if we could have Fred over for dinner sometime after our February cruise. He said he didn't want him over for dinner, but a wine & cheese before dinner would be OK. I asked my husband why he didn't seem thrilled at meeting Fred, and he complained that Fred hadn't asked any questions about us, and only talked about himself, but he was willing to give him another chance. I told him I felt partially responsible because I asked him so many questions. I also asked him why he didn't apply these same standards to one of his closest friends, "Frodo," who always turns all conversations on himself. Unlike Fred, Frodo is usually considered very handsome, gets essentially anyone he wants, and is always bouncing from one man to the next. He responded that he was OK with Frodo behaving like that because they've been friends for many years. So the day for the wine and cheese came, and, hours before the meeting, my husband announced he wasn't "feeling well," and so Fred and I had a wine and cheese while my husband stayed in bed in our bedroom. Fred came over at the conclusion of the hour and told my husband he hoped he felt better soon. I suppose this was a way of "ghosting" Fred. This blocks my ability of getting to know Fred better, because my contacts will be limited to inviting him to one of our summer parties, and maybe going with me to the rare shows I want to go to but my husband doesn't (obviously we go to 90% of shows together, but there are some he can't stomach, such as the Neil Diamond musical, so I find someone else). There are usually other people to whom I'm closer that I'd usually invite, but these would be my only opportunity to maintain contact with Fred. I guess I can't recall I've ever "ghosted" someone before. If things weren't going right, I think I'd try to communicate my needs, and give that person a chance to adjust his behavior. In the case of Frank, I suppose one could argue he was being rude, although I suspect Frank may be on the autism spectrum, and may just need guidance (Frank was on the cruise with a cousin, not a friend or romantic partner). So if you think you're having communication issues, would you generally offer feedback, or just ghost someone?
-
The number of diseases one can get from dirty earbuds is almost countless... 😉
-
What would be your concern?
-
-
You're diverting again (instead of apologizing, as usual) for being FACTUALLY wrong about Zoroastrianism being an official religion in Iran. And the overwhelming majority of nations in the UN General Assembly is hardly the "American view," quite obviously. Without even delving into the facts, if you had known the official name of the country, you'd have known what the only official religion of the country is.
-
Putin doesn't seem to have followed your sage advice. He's been helping the Iranians. I'm sure that'll really endear himself to Tumplethinskin. It might push the rug-wearing thunder-nugget to let Ukraine get more weapons?