Riobard
-
Posts
4,740 -
Joined
-
Last visited
-
Days Won
19
Content Type
Profiles
Forums
Events
Everything posted by Riobard
-
The weather has been glorious but oppressively hot for some. Even the mosquitoes make no effort. Mercury to drop. Transferred to São Paulo for a usual extended Renaissance stay where the temperature reduction brings it surprisingly low but I like it for better personal energy. Enjoy and best wishes for safety, etc.
-
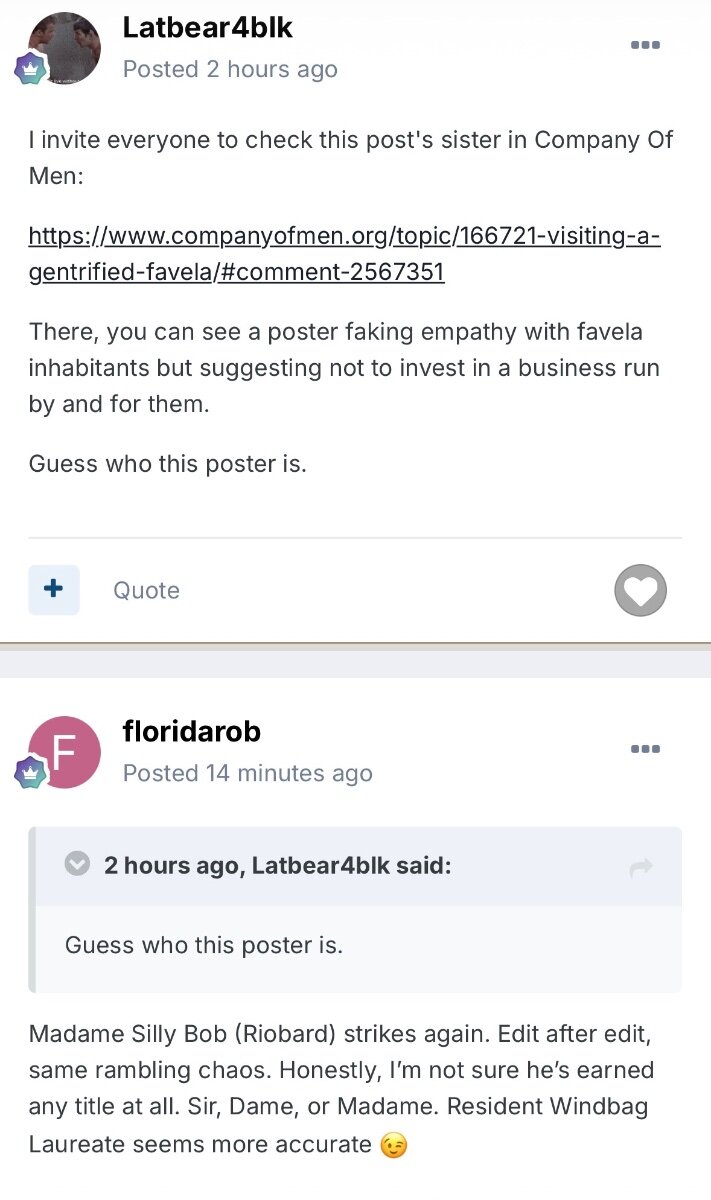
Man, they are as dumb and manipulative as I expected. Here she baits a fellow trollish crony to upregulate in direct sequence the identity speculation and outing of one or more thread contributors, on a presumably thematically similar platform, that chatroom board monitors love so much. So sadly misguided in thinking they have any real troll claw to play. Not sure what “post’s sister” means … sounds like a type of gibberish that characterizes much of her wacky phrasing or sloppy editing. Is that signpost and sine post in a sibling word salad? WTAF?! Now that she has linked new board content, also not sure how to integrate meaningfully the apparent multiple and split personality members of a floridly pathologically dysfunctional family oozing toxicity in chat platform cross pollination, consisting of a bear, a Zé (parrot?) and twin? florid bots? where one was absorbed along the way or simply trades off shifts to explain the subhuman phenomenon of 24/7 drivel? Somebody suggested one of them was muzzled. While understandable, I hope that wasn’t ungracious intervention by anybody I know. Here it is in summary, for a self-aggrandizing insane goof’s reference:

-
Newsflash: Florid Bot wriggles out of straitjacket once again. Proclaims status of friend of friend of friend of friend Plumber? Joe from NY ??? (Next yadaddaddadada blather? for all I know). Presents fake assertion that sending up on our board has expanded from established trolls targeted. Evidences height of hypocrisy when he virtue signals by proxy his friend of friend of cousin 6 times removed that arguably attempts legit good work in a setting from which Miss Bot, when unleashed, nullifies that potential good by selfishly recruiting socioeconomically disadvantaged young men into meagrely compensated sex work, yet melts down when the notion of fair $ transaction is debated. All poor, so should bow and grovel in gratitude it seems. Always able to crank back up from the heap he is. Clarity is what clarity does. The good thing is that this discussion has no impact on the status quo of a decent person’s earnings and any cascade effect of actual good. The bad thing is that this discussion has no impact on the compromised wellbeing of the very lad’s community members/ associates exploited by his … say what now? … friends of friends of WTFKnows.
-
But your tantrums? We’ve got you. You are just persistent, not bright. First image scene blocking.v


-
But for that the toxicity of persistently dumb direction-pointing street drug equivalent Keethquiff may induce uncontrollable nausea among poor unsuspecting servers.

-
Since it came up, 75-90% of the punters at the trade venues might have difficulty squeezing through the aforementioned lodgings passage, but skinny is not required. It’s not clear whether their attendance represents the epidemic of obesity or the brothels are just a particular draw for the physically unwell. Weed does not help the trend. That said, a lot of old sweet disabled men seen there have their shit together better but I worry about their safety navigating enclosed shower spaces without a bench. As important as wifi is whether a shower has adequately heated water. Many don’t and are only more tolerable in hot weather that actually raises water temperature. I currently use the proverbial ‘suicide shower’ in a refurbished place with retrofitted plumbing and electricity powering the water at point of access as opposed to the hot water tanks most are accustomed to.
-
Barcelona - Thermas - Weekend in February.
Riobard replied to hurstwickham's topic in European Men and Destinations
-
Barcelona - Thermas - Weekend in February.
Riobard replied to hurstwickham's topic in European Men and Destinations
Oopsie, he’s apparently about a decade too old and, being fit and muscular, not developmentally adolescent-looking enough for some of the trolls and their $10 trade budgets. But they should be grateful he’d possibly keep his biscuits down dealing with them. -
See “The Rise of Obesity”, brought to you anywhere and in your face. Independent risk factor along with smoking. As obesity contributes substantially to the variance in pancreatic cancer incidence, not that the selected above public figure examples necessarily represents the well established logistic regression analysis for incremental BMI and belt size circumference, then the latter isn’t something that just happens randomly in a significant proportion of cases. Plus there are other benefits to not being obese. Put that in your pipe and smoke it, but really, don’t smoke. Feed the world. Impending downvotes brought to you by mindless self-indulgent troll-marketed dessert buffets as well as troll waist and waste of spaces.
-
Oh really now? I don’t? What a surprise to moi?! A low single digit bevy of wannabe critics with low double digit IQs? Most have pet names reflective of inherent toxicity. Anybody want in on one of the yet unassigned? Factory-sealed mediocrity it is. Starter pack: no original thoughts included. Now includes bonus dumb down arrow emoticon. Algorithmically dumped into your chatroom content no xtra charge.

-
Barcelona - Thermas - Weekend in February.
Riobard replied to hurstwickham's topic in European Men and Destinations
“Eric” is truly hot. Recently I had heard from the hall and from within one of the crap cabins the extended slapping sounds of a groin against a punter’s buttocks as the recipient moaned incessantly. When he emerged I was taken with this stud’s looks. He is a nice guy too, but hard to take😏 Not to be missed. -
Back to the topic … she could put her name in for one of the non-best nights and give the exploited favela trade a break.

-
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
A substantial proportion of uncircumcised MSM indicated a hypothetical willingness for circumcision uptake in the event that HIV transmission risk would be mitigated. The inquiry was posed given that noncircumcision is considered to inflate the relative odds of transmission. Circumcision willingness may depend on subsequently accessible protective factors but openness to trade off foreskin for personal and collective health is notable. Some may had also caught an eyeful of some of the daunting wellness-dismissive trolls, you know, those with the stated entitlement, troll-dolled up as preference, to compromise short- and longterm health for the sake of a developmentally immaturely constructed arousal boost. Cue the pathetic boos and hisses. Losers are as losers do. Otherwise, it is true that there are no data that depict any particular trend related to MSM partner selectivity based on circumcision status. -
Her name? Don’t know. Don’t care. That artificial bacon can say whatever it is; it’s bait not taken. Just don’t call me by her names lest I be conflated with an embarrassment to the blog community. Not that she’s little more than the tiny dot in any com. Already having to repeatedly soap les knuckles, scrubbing vigorously to wash off her radioactive crap. The height of hilarity is that this wannabe critic spinning handles for desperate control would put herself forward as a written content evaluator in any context. Would that the queen store her own dirt under her nails and not drag young LMIC males into a future of rectally displayed regret. [Thanks I that is always me]
-
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
First a pool therapy club with gossamer water wings craning for a gander at the lifeguard they’ll never have, cut or not. Now a poorly packaged misogynistic circle jerk floating in its own incontinence. -
Anybody with half a brain can assess that I had merely pointed out the pathology of a pathetic clown’s identity speculation sideshow. The meltdown is not mine. Her next handle might appropriately be @chernobyla. Her appealing to what everybody would know anyway simply reflects a collapsed claim. One of the stupidest self-serving people I hope to never have to run into and likely won’t. Gibberish? Let’s talk the scrambled logic of blatheringly repeating a disputable fact as if the broken record doesn’t reflect the grandiose impulsivity that set the sociopathic needle down. Let’s just agree that her claim of repeated history plunks her nonsense into the category of folklore bunk. She should stick to the manipulation of LMIC men barely out of youth cajoled by @heavywhinestime into having their sphincters reposted for the dream of a few bucks. The idea that a sad sack crony that also posted her own full name on this board and thinks emoticons are truth social and reflect meaningful reference group consensus has me rolling on the floor though it should be sobering. What a formidable peanut gallery. Next, cue the emoticon of a fugly wannabe daddy ill with the delusion that SEA LMIC men, incapable of sound judgement by virtue of age and deprivation, are actually into barebacking with him. Trump narcissistic, he says fam says? Sure, it’s catching across the pond inn’t.
-
This ought to be fun. OK, sure, own goal Holmeso. Get help. Rehab for the muddle and behaviour mod for Tourette’s-like media stalking. —// There’s nothing over my head here, folks. Go home. I haven’t identified here any equivalent or alternative anonymous social media handle anywhere. I don’t prematurely show my hand. This clown is simply manipulating for control. If they are fine disclosing own handles and true given name, their own images, if that’s the case and it’s their call as to the veracity of that reality, that’s their prerogative. I could care less what they call themselves. What should be of concern is that they would put forward flimsily veiled ominous threats to out others when disagreeing with content, accompanying bitterness with sad attempts at ostentatious know-it-all flourishes. From what I understand, not their first rodeo clown appearance of this nature. Everybody crap at research knows some thing; doesn’t mean they’re bright. When a pathetic punter superimposes their own playbook on their personal identification and their triangulating media handles for troll-ish control that’s when you know the board needs a toxic cleanse, ‘do not cross’ tape at minimum. Take your popcorn and go and enjoy a movie, etc. I personally afford steaming as a result of banking earnings working with this level of sociopathy. Oh and did I neglect to reiterate that the sauna venue grid is a ridiculous piece of crap other than listing correctly 2 of the current 6-7 accessible in Rio? And somebody progressed from their ABCs to days of week? Appended images for narrative effect.
-
I will add, though, that 117 has currently ceased their previous unique promotional discounts for Wednesday. Shifting sands regarding the mélange of fees for entrance, room, and payments by cash or Pix overall wrt their 6 open days. Gone along with social media are the corresponding banner infos within the venue’s inhouse paper and e-posts. That said, again, the day of week has been moot in terms of my visits going on 12 years now.
-
If I weren’t to concede that it’s far more nuanced then slow is the operative term across the board, that is, I accept that I am slow. And when is slow the antithesis of good? I thought it was rapid and that the antithesis of good is not good. More spreadsheet sense for spreadings legs por favor. Tuesday night is the slowest for private space acquisition. What makes extended waiting for your fun and trade deprived of consecutive program earnings a best scenario? It’s best for those that have their symbolic $$ orgasm prior to the suite as a result of the $10 discount. It’s only good for trade if they make contacts for off-site play pay. This isn’t our first rodeo, inn’t? Best for me is attendance without established trolls. Otherwise, no notable day of week distinctions. YMMV
-
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
I take it back. You are capable of heavy lifting. It’s just that you are moving tons of steaming bunk back and forth between a few locations, the latest hooey of which consists of the stupid assertion that a particular region’s clinicians are notable for greed. Go for it, Dronin’ Conan. Enjoy chasing your tail dissecting material and desperate for the last word, and perhaps coming off as manipulative simply because you lack reading comprehension. Meanwhile, I’ll back off as I didn’t realize how much you are triggered. But you may kiss the ring of an old punter magnanimously urging you to move on to whatever life meaning would float the boat of a normal person. I thought you might be having fun but it seems like you are obsessionally overextended here and the reality that you seem to not run out of battery power, however kerflooey, suggests you may be super-or sub-human. Me, I’m enjoying vacay points south, because, well, there is life beyond media. Plenty of hot trade as antidote to chatbot hot wind. I may even successfully cross the troll-infested bridge to add new concrete data and tips that may be of interest to members. Again, to those poor ignorant souls who don’t get it and for whom the only option is for me to swipe left on worth … You may not blow me and I don’t need more reputation emoticons as they all cumulatively denote positive status. You are welcome for those I provide that confer the same quantity uptick. -
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
-
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
It is said “Don’t meet your heroes”. However, do become personally acquainted with the pill that you originally thought encapsulates your worst nightmare of a troll, but you end up on the floor handsomely laughing your ass off realizing that her misplaced confident hubris is an artefact of chatroom media dynamics and its flimsy curtain.
-
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
This frantic ranting seems very very very uncut. I’d exclaim “Smash cut!” for your own benefit but who’s to stop you, a reasonably smart person (bot?), from decompensating as you seem to be doing here … and who is to stop your cronies, given who many of them are and well beneath your level of intelligence, from paradoxically exacerbating how inane your entry is. If you want legitimacy it doesn’t help to have dumb, dumber, and dumbest proclaim emoticonically “Yup, what he said.” when that’s all they’ve got. And by the way, I’m financially well off and have 100’s of thousands of extra dollars, that I’ll never deplete, to spend on hot trade as a result of my academic writing skills, including having single-handedly secured a government wage compensation package worth collectively millions of dollars for a unique disenfranchised professionally accredited working group of about 5 dozen. I took a week off without pay to write it, met for two hours with gov’t executives, and took only an equal cut that nevertheless cumulatively yielded hundreds of multiples of the paltry one-week wage loss. Other pay equity working groups were begging for my template. I have also published academically on invitation, not subject to peer review. And I think I’m average. Cue let’s see what predictable stench blows out of trolls arses going forward. -
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
What a fun gayly run on desperate attempts at product R&D for a board-based “Devil’s Breath” version. Word to the wise, trolls and a meagre and meaningless batch of wannabe street drug dealers … not drinking your Koolaid. Yawning anyway.