Riobard
-
Posts
4,740 -
Joined
-
Last visited
-
Days Won
19
Content Type
Profiles
Forums
Events
Everything posted by Riobard
-
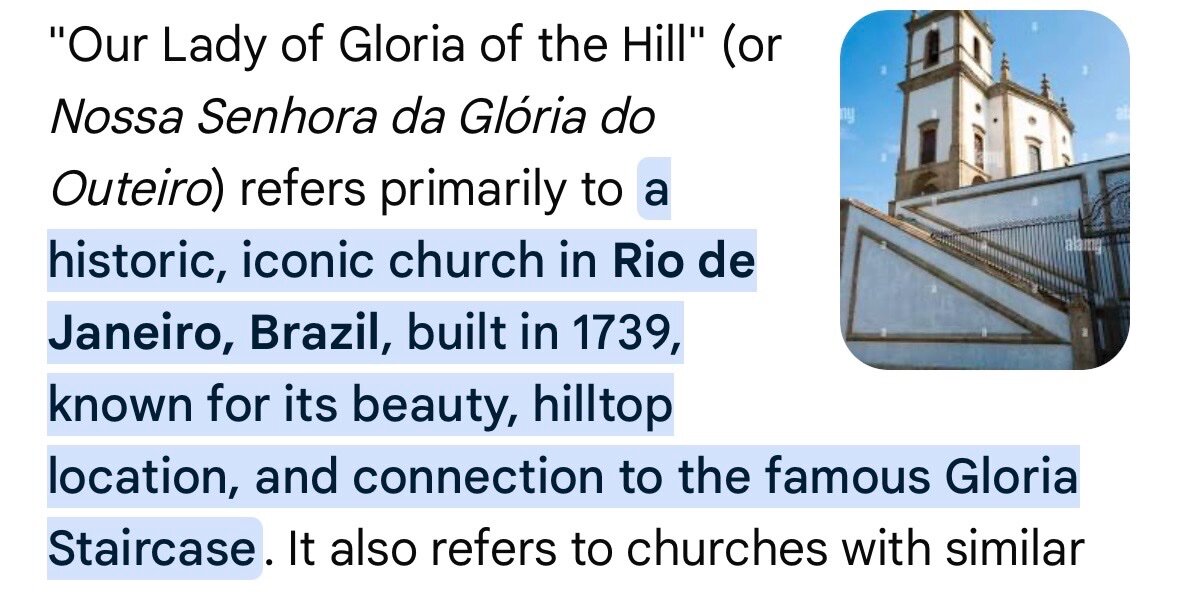
You packed a lot in, impressively, over 9 days considering feeling unwell for part of it. If you missed it, literally steps from your lodgings, long staircase by Golden Park or winding travessa option, try to get up to the lovely church (c1734?) for the architecture, tiles, and view. Sunday morning a good bet to see inside prior to the nearby vast market.

-
Getting ready - gathering up to date recommendations
Riobard replied to GoldMember's topic in Gay Thailand
OK, I give. What random word salad isn’t the core of your content? You are clearly at your best trolling, albeit unsophisticated. Just do that. -
Is this an excerpt from a short story that actually makes sense?
-
WTAF?!
-
Hunh?
-
You’re beyond any.
-
That’s exactly the type of response that coheres with my appraisal. Again, ask her, but fill in the blanks.
-
Right, because a skinflint always possesses the most precise assessment of a cheated person’s affect.
-
Non-manipulation SVP.
-
Unlike here, the protocol for handling narcissism that comes a clinician’s way in a treatment context is quite different. I am also, paradoxically, getting paid to be respected and the fee is much higher to be a sad sack’s punching bag. Toxic costs more. They are paying to do some work in good faith. Somebody like you? … I’d perhaps find an excuse to not accommodate, even if it meant a white lie regarding my own adequacy. One or two per year maximum quota. The lawyers, for example, in my practice have been typically respectful and rewarding. You wouldn’t find them trolling in a desperate ploy for relevance. Anonymity alters the picture both in terms of personal comportment and style of language. Lawyers in opposition and adversarial, in contrast, for example in a sitch of expert testimony, have been put in their places. The dynamic and exchange obviously contextually differs. I have been consistently disabused of the notion that they are particularly intelligent analytically or correctly anticipatory regarding opponents’ ability in relation to the subject adjudicated. But many are reasonably bright and often have unfamiliar curves tossed at them. Their level of deference is moot and likely cloaked in resentment. I’m not completely sure of your background but I’d say you are pretty easy-peasy to compartmentalize in such a way as to amputate from day to day consciousness. You’re the guy with a low single-digit array of lazy retorts. I would never explicitly formulate “Asshole not specified” although it colloquially fits in some instances, and your relation would grasp the wordplay, perhaps even chuckle. Ask your in-law for translational guidance without necessarily revealing the players. That said, a family member essentially has hands tied not knowing all of the behavioural aspects of an aging geezer punter oriented to, say, seeking unprotected insertive anal intercourse with naïve and physically poorly developed and socioeconomically deprived young men abroad for pay. That might partially trump any misguided personal regard heretofore displayed. Only you know for sure what about your number fits the scenario. There can only be bad or neutral sexual tourism. Good sexual tourism is a misnomer and most patients, lawyers, clinicians, etc, would agree.
-
Perhaps I’ll never learn. Take the first text pass as a clue to the mind numbing to come. Take the lame critic’s fallback urging uptake of psychotropic meds as predictive of drivel. But on that very subject, appreciate his stimulation of marketing creativity: “Keethqueef, the hot wind beneath your wings”. Ask your in-law why you refuse to ignore content you find disagreeable while proclaiming to block me. Obsessed much? She has her work cut out, all DSM axes, inn’t? The most basic can seem the most complex.
-
Just helping you release your inner troll tension. More altruistic than fun. No, strike that a little; each time dealing with your ilk adds extra self-efficacy. As far as incomprehensible nonsense just read your own topic. The majority is “in” commentary. Is it a drunken dinner party transcript? Just clarify from the outset so as to offer a take-a-pass option, or a glossary for those with time to waste. Sheesh.
-
I can skate a rink circuit but the best musical accompaniment to a program, if I ever attempted one, would be ‘London Bridge is Falling Down’ for the short and ‘Husha Husha They All Fall Down’ for the long.
-
Decoding anybody? I have been to Bangkok. Most of this would have dissuaded me from visiting but I quite enjoyed the several interesting weeks there.
-
I follow skating enthusiastically and have met a few notable Canadian competitors socially. My peers and I don’t objectify skaters based on physical attractiveness factors. That level of commentary is just dumb, contextually. The spoken word poetry in Malinin’s music has been criticized in some camps but I don’t mind it. It might be deemed too ‘precious’ for a less stellar athlete. He and Hanyu have in common excellent Canadian choreographer Bourne and there was a brief slow sequence some years ago in Hanyu’s program that mesmerized me. Looking forward to the Milan event. I watched Ilya thru the recent circuit with NBC commentary due to my location. Johnny and Tara try to bring a little bit of fashion fun and flare and play well off of each other. It is nonessential but otherwise broadcasters tend to simply list off jumps and rotations. Weir would be brattier if he were to be given more rope. I will prolly tape both American and Canadian broadcasting to amputate the approximate 40% of time riddled with repetitive commercial breaks. Right now I’m in 35 Celsius weather but will be back soon in a state of freeze and the Olympics will be a welcome treat by my fireplace, bridging the span to a subsequent ‘snowbird’ trip.
-
Hahahah … I was wondering when the panic would set in as it’s down almost 2 weeks. In short, to be reinstated em breve. I think it will be a reset without the post history. There have been a few other changes too inconsequential to list, not that any represent improvements regarding the venue’s deficits. These things sometimes occur when nobody is designated as backup for accounts and passwords and the social media organizer has moved on. IDK in this case. The onsite A/C bar screen ads are reinstated, I would surmise a harbinger for Instagram, X, &c reappearance.
-
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
Like the man said. The notion of deprivation is primed more robustly when something is taken away, but it’s both a flimsy argument and accompanied by the absence of comparability in such a way as to circle back to the deprivation narrative. That additionally contributes to the perception and assertion that the practice is essentially heinous. Yet if it shoulda coulda woulda been limited or restricted there’d be no additional data to support the same idea regarding sensitivity and function. Only a ratio shift in terms of the circumcision binary. An extant sufficient proportionality among billions globally has yet to yield consensus. Anchored beliefs are hard to crack. We know this as well based on other platforms whose language and imagery supports the concern that paedophilia adjacency is subtly if not overtly endorsed to the extent that interested members are turned off and refrain from explicit descriptions of trade experiences due to the risk of inadvertent association with perversion. -
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
Try not to get too sucked in, @unicorn -
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
That you describe it as mutilation is a thing. I need to know the BMI of anybody weighing in on this topic … that and other adult variables influence my response. -
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
I find the difference impossible to gauge due to where the member is predominantly positioned. -
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
Just over 17? One would think some think it’s more flexible. I’m not one of them. They are also sad cases hiding behind an arbitrary age setpoint when some areas of autonomy are undermined by the expediency of access to life’s necessaries. Forced choice. As you know, and as some sex tourists integrate sensitively into opportunistic play. -
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
I haven’t met a circumcised man in my personal life incapable of robust orgasm. I have met uncut men incapable of arousal and orgasm. I haven’t treated a man in my practice who proclaimed an association between circumcision status and sexual response … yet inquiring about sexual function was boilerplate in my practice. The substantial majority of men in my practice presenting with function concerns had exercised the adult autonomy of doing shit do their bodies. Some went on to pursue major invasive surgery, costly rehab, etc etc, in attempts to mitigate the sequelae of that shit. I have about half of foreskin tissue residually present at about complete lower circumference, a little less aesthetically idiosyncratic than if it were 21:00-03:00. The northern boreal doc must have been abruptly called to an emergency mid-procedure that left my southern half unexposed. Not one iota of sensitivity differential. Sensitivity is too uniformly high to discern a difference. I don’t add this to make a case, as anecdotes aren’t worth the splash of half and half in your coffee while the trajectory of my emissions is not governed by hemispheric variables. -
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
-
UK to Consider Male Circumcision as "a potential form of child abuse"
Riobard replied to PeterRS's topic in The Beer Bar
No, in fact, what a boring vocal minority and pill you are, still trolling here, generic Aubnocksius, brand Ahzwhole, streetname ‘Keethqueef’ for its noteworthy hit of induced boredom. As well as an apt intrafamilial reference point for an inlaw’s take on a presidents’ personality. Yet easy for any smart person to exposed to metabolize. Nice try to distract from your actual relatability to the topic and reality that the proportional age-associated weighting of your personal genital observation in a LMIC would add another layer to her psychodiagnostic formulation. Tell her I had a Keethqueef slipped into my caipirinha and see her knowing nod, the one distinct from nodding off to the Nobody 1 & 2 film series streaming on Apple. -
IDK, but former club dancer and sometimes sauna masseur (non-erotic) gives a decent rubdown. https://www.instagram.com/massoterapeutariodejaneiro?igsh=cWxwMzBtdTY1Mmsz