Riobard
-
Posts
4,740 -
Joined
-
Last visited
-
Days Won
19
Content Type
Profiles
Forums
Events
Everything posted by Riobard
-
short Jan Brazil trip report
Riobard replied to babybear2's topic in Latin America Men and Destinations
They didn’t think you were florid enough? ;>D -
Must be something in Canuck tap water cuz I totally identify with your narrative here. Manny’s inventory tends to be more reflective of the genital endowment aspect because that seems to be the predominant ask made by visitors, but that is not an important feature for me and I believe he has somewhat stereotyped tourists’ desires according to the trends in what is appreciated and requested. There is not much of a range in categories of types because his profit margins are geared more to a relatively constricted somatotype, or so I think based on one visit and on what has been illustrated in his photo catalogue or by other members here. I can more easily get off with a physique model type that keeps his panties on! So my martyrdom regarding inches is perhaps somewhat unique, some might say eunuch lol. He knows a lot of those guys and attends competitions as a spectator but my sense is that he tries to keep things compartmentalized and not attend the same gym workout circles as his supply chain of dick. And then there may be a phenomenon of, ahem, price-point adjustment. I don’t mind because I have ample funds. I just don’t want to waste time trying to get good matches or be breaking in a newbie figuring out whether he wants to branch out into the trade to support training costs, etc. And I may have left Manny a bit frustrated too though I thought he was trying to be patient and accommodating. My willingness to raise the bill and his profit margin did not yield much. He is just more accustomed to running a quantitatively high output low-ball$ big-balled shop. He may also be puzzled about the MSM brokering niche because he probably gets a ‘pussy is pussy’ vibe from his straight clientele and finds guys like me too finicky … and how can I be gay and not just be satisfied with challenging cock?! The thing is, my type is readily accessible in Rio, so it’s not really a question of my tastes being particularly unrealistic or demanding. In terms of pictures there is likely a somewhat greater down-low aspect to the types we like so I wouldn’t expect an advance catalogue to be forthcoming from him. I also have my doubts that Ezequial’s supply chain is an EZ prospect for matching. It may be more along the lines of the ‘sanky-p a n k y’ trade for mature ladies. I will likely eventually take another run at Manny. He is a fun character to be sure.
-
I would expect such an off-point response because I did not anticipate a course correction. This isn’t truly real life since my sense is you readily create rabbit holes to fall into … read the room. And read an editorial or two while you’re at it; you may find that written word deviates stylistically from spoken. BTW who uses the wording “quasi-gay” in real life? When you’re reaching out to providers here, best of luck conveying your specifications concerning the antithesis of such a peculiar term. LOL
-
Any suggestions for waxing in SP
Riobard replied to topjohn5's topic in Latin America Men and Destinations
It’s been a while since this type of service info was updated even a little but I was somewhat on top of it investigating more the ‘tantric’ side when there recently. Grand Spazio, conveniently located near Ana Rosa metro station on both blue and green line. I have not been there but it’s also close to InHouse Agencia where I recently had one of the hottest tricks of a decade, skipped the massage part and into full play BRL250 for one hour … he pays the house a cut. In my home city that gets you about 6 minutes of lap dance. I had dropped in for a tour & when I left serendipitously saw a guy walking on the main road that made my knees buckle so I followed him, and sure enough. He removes his mask once I followed him up to reception and I die again, then his personality a 3rd death … and so on eventually to a big petit mort by appointment the following day. I had expected massage with rub-and-tug HE but so much more exciting transpired. But I digress.
-
What I noticed, @topjohn5, and similarly if you indeed noticed your own post history, was a rather fragmented list of topics/questions on your part, most of which already have oodles of extant answers on this board, as well as your input viz your preferred “type” (usually vague at best and that goes for everyone) … then recently an implicit grousing about whether you would find them other than at escort sites. Since the very few sauna venues is such basic info and I actually read your other posts, how actually off page was I being in attempting to integrate your agenda clues and offer some direction, in thinking about making an effort though actually rather futile to stratify venues in keeping with your general sexual interaction goals? But then I made the effort to grasp your playbook, to be hospitable, while it’s apparent you might want all the info repeated on a silver platter rather than taking a few very worthwhile hours to gather the reams of info at your fingertips here to help you curate your visit. And yes, hours, attributable to the phenomenon of groundhog-day infinite repetition of the same questions and over-accommodation in the same answers. This over-accommodation by some paradoxically enhances the daunting prospect of a one-sitting scroll-and-discover on the part of newbies. And lack of consensus about material organization just exacerbates it. Thank Gawd for the pandemic in this regard offering redactive respite. Then you further define the exact terms of reference for a contributor to answer an open-ended question after the fact. Sheesh. Good luck with your trip. Or should I perhaps say good luck to the horizon. I unexpectedly discovered the closest to the (your) real thing this weekend, as my blinders typically screen out particular inventory types, but there are too few venues to prevent tripping across it and a turned up nose might be the anticipated response given some of the general provider criteria you alluded to. I suggest you read the relevant site topics and later pound the tiles with your flip flops like the rest of us, the hunt sometimes half the fun. You’re not the central character in Death in Venice so it could be a good time.
-
Oh, dates lined up with twinks that are more homosexual than “quasi-gay” [sic], I believe? I wouldn’t particularly recommend any single sauna venue so the details of those places may be moot and the type prevalence is not very much matched with specific nights. The same types of providers proliferate across time within a given venue.
-
…
-
The two in São Paulo and three in Rio de Janeiro all have Instagram pages that are generally a good up to date source of info, events, etc. These pages are not necessarily all operated to the same standard but give a fairly accurate picture. It takes but a minute to rifle through all five in one sitting. Why seek opinions about the best where’s and when’s? So we can read them over and over and over and over and over again.
-
Obscure transport question SP beach cities
Riobard replied to Riobard's topic in Latin America Men and Destinations
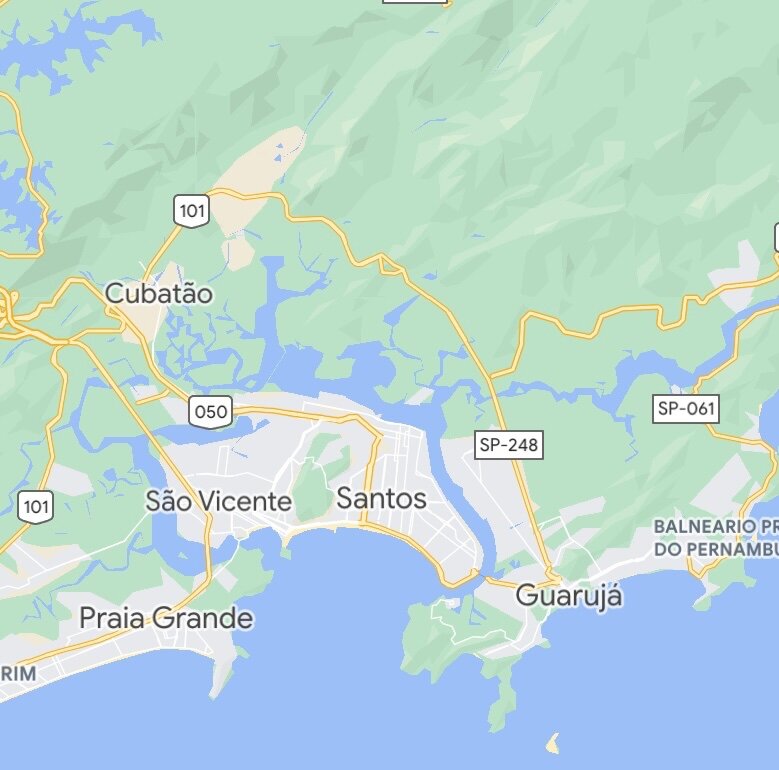
FWIW, though the ferry service site mentions only vehicles and bicycles, I recently discovered pedestrians may cross. If you are involving a ride service you would need to allow for the driver to wait and cross (at what price?) or do it in two stages. If you have long stay time on your hands a trip to Santos bus station (from Jabaquara Metro and it’s attached regional bus station) to visit the coffee museum and have lunch is a pleasant excursion. The bus is 70 minutes each way, dirt cheap, some dramatic scenery closer to the coast and glimpses down the estuary zone of huge swathes of beach high rise real estate. WTTW you do need to produce your passport for regional bus tickets, any private bus company for that matter, say, to Rio. The museum was the only place over a full month that requested CoV vaxx proof. Same idea bus service to Guaruja and other more beach-y points south. Personally I think it’s easier to pick between Guaruja alone by bus, or alternatively among the few points west of it, to avoid ferry crossing during any one excursion. One or the other zone different trips, as they are not huge distances or travel time from SP. -
São Paulo very much permanently in the rear view mirror. Not enough rear views to my liking.
-
The part about douching spoke to me. I brought supplies for 4 wks Brazil recently but could not muster the will to utilize. In 70th year but fortunate to have robust tumescence, perhaps partly owing to lifetime healthy nutrition and exercise. Fortunately, about 90% of the time no embarrassing GI-related mishaps upon protected RAI when attempted, and simply avoided or truncated when I thought it might be on the messier side. On a side note, I was violently ill vomiting one day and my tentative conclusion was it followed 2 strong caipirinhas of an evening at Lagoa early in Truvada cycle after having 2 years abstention PrEP. So later re-challenged but then abstemious re: alcohol. I don’t think it was food poisoning. I am not much of a consumer of alcohol ordinarily but was essentially mildly drunk on the cocktails.
-
Omicron CoV VOC Brazil, etc
Riobard replied to Riobard's topic in Latin America Men and Destinations
Very prudent, if you have the flex to defer and your balanced assessment of personal risk is that avoidance of CoV infection is paramount. What I can tell you from paying attention to some of the local news is that the science-based pandemic management table here is advising a renewed Rio ‘lockdown’ but that will likely not materialize owing to reluctance to again endure the secondary impacts we know to be characteristically problematic viz economy etc. The air is microbially dirty; it’s the new poop. The more people congregating in any human context the bigger the bugger deuce, metaphorically speaking. By now everybody should grasp that observable pandemic mitigation infrastructure and implementation is not a reflection of case incidence and the accompanying risk of infection that necessitates medical intervention for a subgroup of infected. -
3 years ago the baths bartender was stunning but aloof. I would have thrown money at him if given some encouragement. But I would wonder how he could cover all stations. There was an undie shop at the front but I don’t recall if it was separately staffed.
-
Sao Paulo newbie AirBnB question
Riobard replied to topjohn5's topic in Latin America Men and Destinations
I always carry a reasonably decent decoy phone and decoy $bill/card-fold that are both essentially dispensable and in my outside lightweight full-length pants pockets where I hope a thief would consider the logical place for a pedestrian to store belongings but not, to date, any encounters such as requests or demands to have them removed from my person. I assume, possibly falsely, that a robber would not stick around long enough to inspect the contraband. The felon would quickly see some cash tucked into the cheap wallet thingy. The hope is that would be an acceptable tradeoff for my personal security and life to remain intact. My undergarment is a bathing suit or lightweight shorts with pockets where I fold up and distribute some higher denomination cash and functional credit cards. Usually at least one large enough pocket in the undergarment to conceal my true phone. Essentially I would need to be frisked to reveal these genuine valuables. -
Apolo … been there dump that; not appalling, but … ———— Juan Bin Bin … Bin there dump that. Don’t wanna go to there again.
-
Meat Loaf, latest anti-vaxxer becomes victim of his false beliefs
Riobard replied to unicorn's topic in The Beer Bar
Grave worm chow alert: Meatloaf special this week! Messenger ribonucleic acid-free! FullSizeRender.mov -
Chatter = “Ele não embalou seu equipamento de autoasfixia junto com seu nitrato de amila e tudo o que temos a oferecer é um pouco de plástico.”
-
Watch your phone in the Sauna!
Riobard replied to Traveler365's topic in Latin America Men and Destinations
I am neither a phone lover nor at all umbilically tied to mine beyond the basics of postmodern convenience. Or necessity, eg Über in Brazil. But if you haven’t been to, say, 555 on a Friday night prior to the late evening stage circus you haven’t experienced the equivalence of essentially watching paint dry when you could be catching up on written word news, other reading, etc. If you haven’t laid eyes on your new obsession, IMHO these environments are among the least interesting and stimulating settings I have encountered. Of course, there can be exceptions where at times things get more dynamic, even outside the tricking component. But phones are the new books at those times a Plan B comes in handy while biding time. And I am someone that can happily sit on a nice park bench in a regular square for long periods of time without being glued to my device. -
To navigate via ride platform(s) between Guaruja and points west, and vice versa, Über to short ferry and complete the transaction, cross as foot passenger and order a new ride, correct? To avoid the very long circuitous route points north and so as not to unrealistically impose on a driver to navigate the crossing? I tried to use Über estimator without success. Maybe somebody knows. The only reference on our board was a traveller with a private vehicle utilizing the crossing which I understand to be no more than a few hundred metres.


-
That’s not a stretch. And it is a stretch.
-
Omicron CoV VOC Brazil, etc
Riobard replied to Riobard's topic in Latin America Men and Destinations
Thanks, it’s a bit misleading due to surveillance methodologies in Brazil. 95 Sunday likely a data dump of several prior days where reported incidence was in 0 range; essentially off-duty sitch. 16-17 Monday (as in this table) perhaps reflective of trend of day of rest affecting reporting. 35 Tues perhaps another retroactive catch-up from weekend. Remainder of week could tell the story better. The astronomical percentage increases in the table are also reflective of previous testing hiatus situation many regions. The true 14-day change should eventually be better representative of reality in a few weeks if testing and reporting stabilizes. But the temporal curve trajectories tell that part of the story as well. Hospital admissions a good indicator as population testing accuracy, as you know, has thrown up its hands. -
Omicron CoV VOC Brazil, etc
Riobard replied to Riobard's topic in Latin America Men and Destinations
So now São Paulo city and state COVID hospitalizations have quickly jumped up to 25% the pandemic peak, when the situation seemed dire. This current trend does not appear to abate, and this is a context of very high levels of full vaccination, unlike said peak of Spring 2021. Less disease severity coupled with higher case incidence, albeit proportionally less CoV morbidity, does not portend less strain on the health care sector or improved net absolute population consequences unless the Omicron variant quickly burns itself out. -
Sao Paulo newbie AirBnB question
Riobard replied to topjohn5's topic in Latin America Men and Destinations
@Novarunner, do you know the app Subtitles Viewer? You can sync written subtitles to just about any movie or TV program. You won’t get the auditory Portuguese language but you may find it useful to see the text play out in concert with English soundtrack.