Riobard
-
Posts
4,740 -
Joined
-
Last visited
-
Days Won
19
Content Type
Profiles
Forums
Events
Everything posted by Riobard
-
Domestic airfares in Brazil - why so expensive?
Riobard replied to speedoo1's topic in Latin America Men and Destinations
I got a sealed cup of water from a dispenser on the bus in Brazil, not that I would want to stim my bladder to have to use the toilet. I must have slept through the gourmet meal service. LOL. The lie-flat did not suit my 6-foot frame because the angle is such that the middle part is slightly convex and the foot part drops down, so there is ergonomic pressure pushing up into the lower back. Passengers talking loudly and incessantly on their phones rather than texting, waking me up in spite of noise-cancelling earphones. Some watching things on devices without headphones. We live in an age of shared-space etiquette absence. The consolation is the bus travel savings covers one or more hot fucks at one’s destination. -
Domestic airfares in Brazil - why so expensive?
Riobard replied to speedoo1's topic in Latin America Men and Destinations
As suggested, the bus as an alternative. I recently paid $20 USD one-way purchasing the day before. Early morning departure Rodoviário Tietê (São Paulo Metro’s blue line) … Rodoviário Novo Rio (beside light rail transit station connecting to Rio’s Metro) … to dovetail arrival with accommodations check-in. The buses were full so buying your ticket at the station sales desks just prior to boarding may be a problem or leaving you to scurry around different carrier queues. I took the company ‘1001’ but I think it is a division of ‘Cometa’. Seat is assigned so you can show up 15 minutes ahead for boarding, that basically cuts the flight travel time differential, avoiding check-in/security, down to some 5 hours but you are essentially paying yourself $20-40 per hour to relax, view downloaded streaming etc. Bags are tagged as they are loaded by staff; no overhead bins. If you make a trip to the station on a separate day to buy from a desk rather than online, you need to show your passport as you would boarding as well. I am not up to speed on local transit ticketing as I ride free and it is often as convenient as Über, seeing as I stay near stations. Years back the light rail transit in Rio required a different fare loading card than the Metro system. Therefore, it might be advisable to make a trip ahead of time where the light rail transit above ground (VLT that also serves SDU) connects close to one of the Metro underground stations such as Carioca or Cinelândia where I think you could obtain (buy?) up on the tram platform a loading card. I think cash is the method for buying fares on the card; I recall putting bills in the slot and I think I strategized amounts as I don’t think it made change. Anyway, you then have the card permanently for future use rather than being caught unawares if you did not account for this step getting to the bus station. Not for the faint of heart if loaded down by luggage though. -
In the perhaps inevitable SNL skit I wonder if the post-sentence verbal dust-up will include: “You think we don’t know that’s a rug?! Who do you think you are, Corey Feldman?!”
-
Austrian Movie Great Freedom Opens
Riobard replied to tm_nyc's topic in Theater, Movies, Art and Literature
Oh good. I can see it this coming Friday or weekend a few minutes walk from my home, and The Worst Person in the World today. It’s been over two years since attending a movie theatre and not all international films end up on iTunes. -
I went seeking NOT a massage with one of the guys that I met there a day before that had just come in as I was leaving after I had dropped into reception to view the team photos, but he was booked at that moment and not available. The next day at my appointment with him I anticipated (was resigned to) massage with happy ending BRL250. That was going to be fine because I thought he was at the 95th percentile in attractiveness across dozens of sauna providers I tricked with over several years and I am typically satisfied whatever the depth of sexual interaction if it is someone that is an absolute must-have. But I was upfront and asserted that I would prefer to get into sexual play immediately and skip the rubdown. He was very obliging and said sure we can get right into it, IT being as it turned out the full sex script characteristic of sauna brothels, for an hour same fee as quoted for tantrica. 5 stars. My sense is it is not the standard and the set payment may get you a range from mild to wild depending on the guy; the venue not involved in the hierarchy of perks provision. Interestingly, he was unfamiliar with Lagoa although Paulista and I don’t think he was taking a piss. Seemed educated with above-average English proficiency relative to club escorts.
-
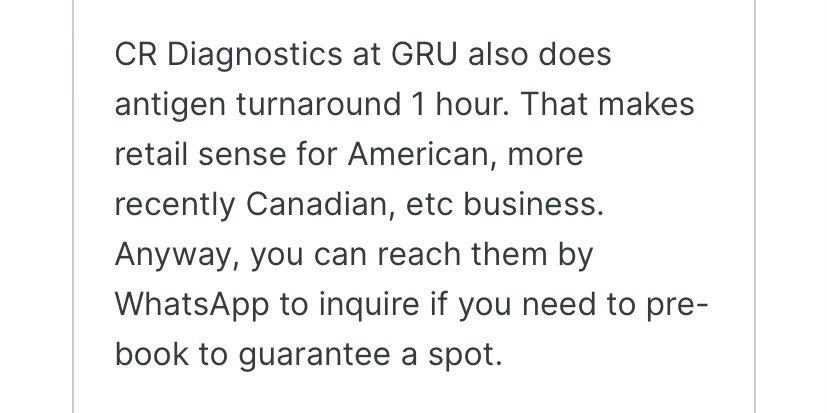
That’s a perfect strategy as you are at the airport anyway. I did it in Rio south zone because I took the bus to São Paulo centre a day before leaving from GRU. It will likely be CR Diagnósticos at Terminal 3 Departures. Make sure the person creating your case has entered your phone number and/or email correctly so there is no drama getting the results electronically.
-
I usually get the ‘something is wrong’ notice but I am logged in successfully so I just ignore it.
-
-
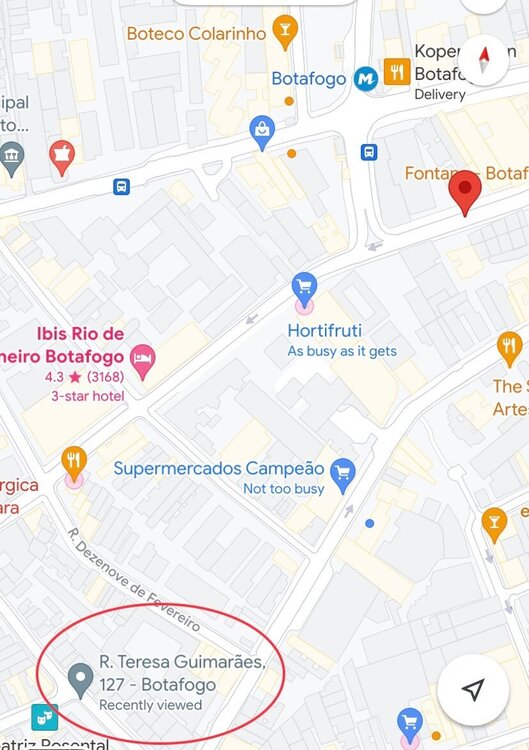
There may be ‘method in madness’ so to speak, but why? To get a result while waiting hours way ahead of time to board same day? A commute all the way to GRU and then back to the city for the sake of a swab a day or two ahead of day of departure for USA, for piece of mind? There MAY be easier options in the city or, in fact, if you are going from Rio back to São Paulo and wish to go the molecular test route that you can obtain in Rio, rather than antigen, for USA entry, depending on layover duration in São Paulo. But beware because the turnaround time in Rio in the city is long, except for Laborlife. Obviously, I don’t know all the testing centres but stayed with Laborlife because it’s convenient and reliable. However, LATAM suggests CR Diagnostics at GRU and turnaround is up to 4 hours, while its branch in town Mooca is apparently 24-48 hours for results. However, I think you need to book the test ahead. It makes sense for there to be a collaboration at the airport, but all that extra time to kill pre-boarding, ugh. And pre-booking likely reduces the chances of a Hunger Games scene on walk-in basis. Stress. I would be inclined to make the commute trip to GRU but on the day before flight if bookending the last part of the trip another stay in São Paulo. Personally I’d just take the Metro. Laborlife in Botafogo is a sure thing for 6 hours (or cheaper for 12 hours) and getting that done in Rio on walk-in basis worked perfectly for a departure from São Paulo 2 days later. Timing is everything. For antigen tests some members have suggested drugstore walk-ins but I tried for fun and was told they no longer do them; may be an artefact of approval of home RATs as of end of January. Outside of travel I expect locals prefer cheaper DIY kits they can purchase without the pharmacist doing the swab. Laborlife does offer it supervised 2 hours for results but that might be viable for a same day flight from Rio or from São Paulo if you get to GRU the same day.
-
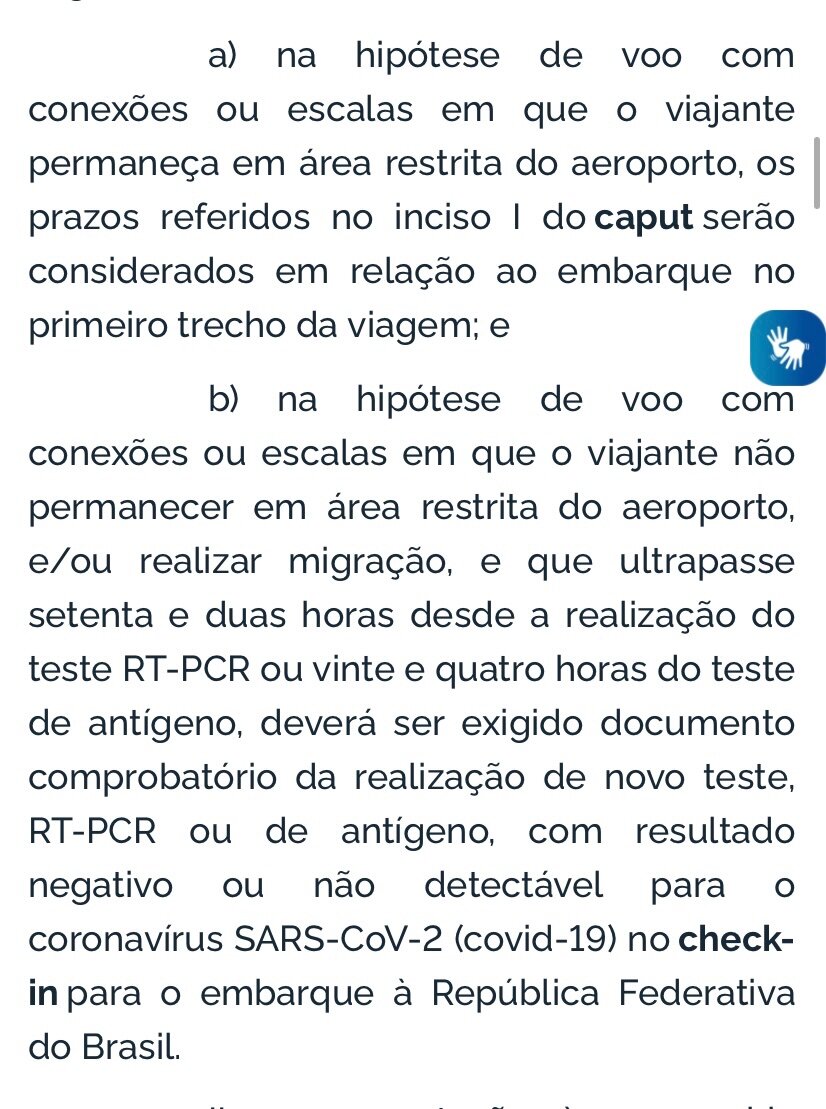
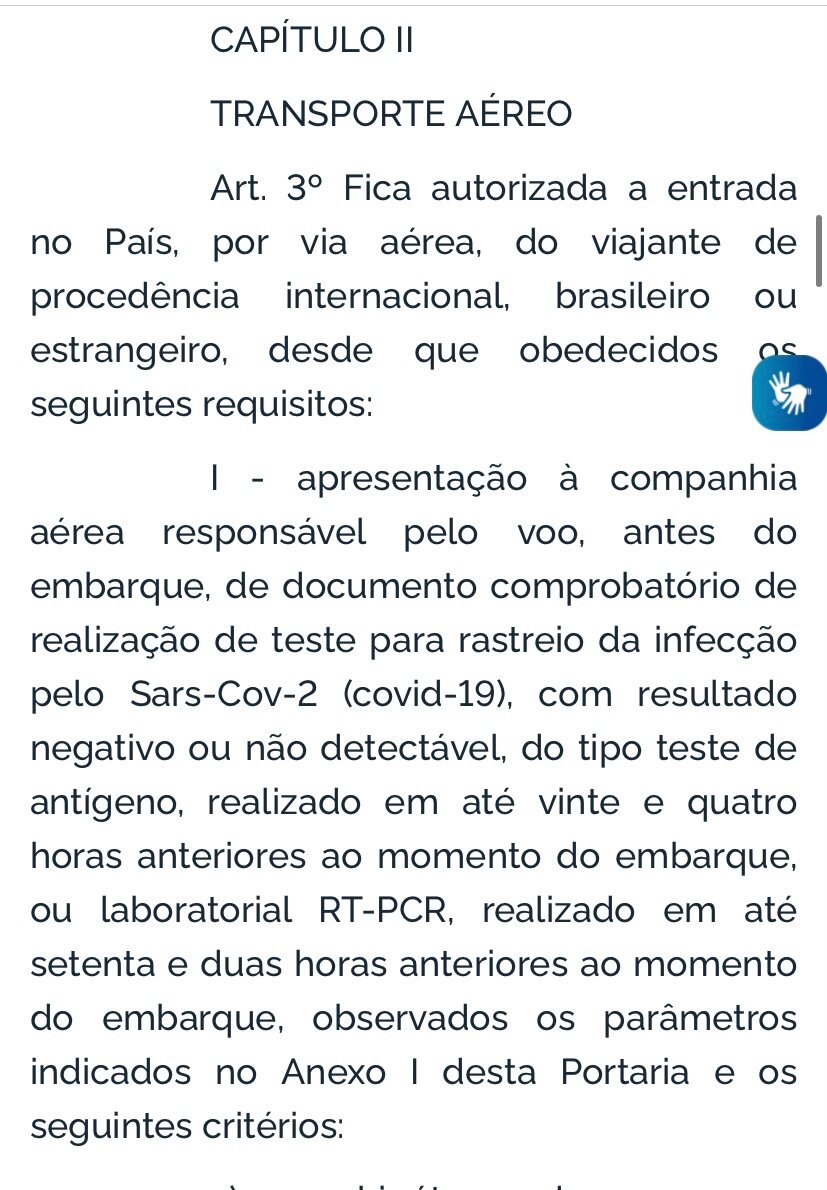
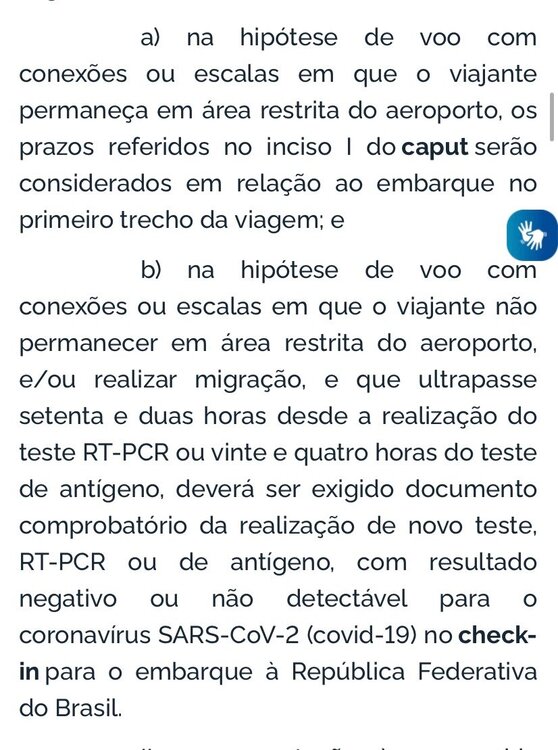
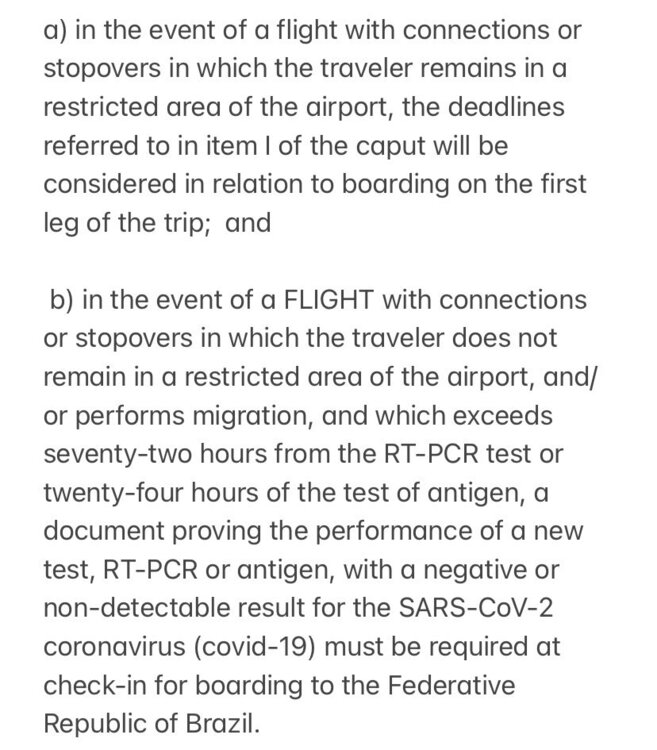
Here are the original ordinance snippets of January 21st in the event you need to stand your ground and school the checkpoint officer on arrival.
-
2) Not for domestic travel, ie, a completely separate short haul, say, predicated on staying in São Paulo initially. If it is a through ticket from São Paulo to Rio extending from USA boarding I think if I recall correctly you clear immigration at São Paulo so that the stopover/connection clause above does not apply within Brazil (in your case a second connection). It’s been so long since I did an immediate arrival connection, but I am fairly certain I officially entered at Terminal 3 and rushed to Terminal 2 for the domestic flight. Incidentally, arriving in São Paulo this year of a morning was very quick disembark-to-curb with COVID test/vaxx and passport checkpoints.
-
For (1) see attachment below, a translation of the ordinance. There are also misguided travel information sources that indicate 24/72 hours respectively prior to date of travel. It is actually time of flight. If you ask me, there remains ambiguity. I would prefer to arrive in Brazil within the time frame from actual swab collection, 24 hours or 72 hours, to avoid hassle. I think an antigen test in Charlotte on a Thursday and boarding in Charlotte on a Friday might pose a hassle on arrival in Brazil irrespective of remaining airside in Miami, IF swab to touchdown lapse considerably exceeds 24 hours. I find that the RT-PCR test confers more flexibility for unexpected time occurrences. I also do a home-based rapid antigen test the day before the molecular test to reduce the chance of an undesirable impromptu surprise. Also, remember to complete the Traveller’s Health Declaration within 24 hours of boarding. ——-
-
Barcelona (Thermas) 2019 latest recommendations
Riobard replied to joe2001london's topic in European Men and Destinations
Also be aware of prime series vaccination expiry status, 270 days, unless you received a subsequent accepted booster dose, or I believe proof of infection recovery following prime series, that infection also perhaps having having a lapse limit. I reviewed this prior to booking for an upcoming trip. The above details do not apply to me, so I am not particularly paying attention to them. In contrast, Switzerland just removed these entry requirements, so places like Spain may follow suit going forward although its expectation for a booster dose for many visitors puts it higher in the requirements category. -
First time in Brazil - Rio, SP and ???
Riobard replied to Taikonaut's topic in Latin America Men and Destinations
Recent reviews of the luxe Belmond Hotel in the cataracts park, where guests can optionally access the falls before and after regular hours, revealed no disappointments from contributors. But here is my photo montage from a Fall (Spring there) visit a few years ago. It was not a dry spell and likely more flow volume than recently but I actually wonder if the more forceful tracks are muddier due to more riverbed churned up. I was surprised at the ‘cafe au lait’ tones. Looks like a 🌈 can be pulled out any time kkkkkk. FullSizeRender.MOV -
First time in Brazil - Rio, SP and ???
Riobard replied to Taikonaut's topic in Latin America Men and Destinations
I suggest that you feel out your initial location Rio and make decisions about a third destination while you are there, or even from São Paulo your second location. Rather than commit now and risk being squeezed for time, that passes quickly. While recently there for a few months I made 4 impromptu changes related to location and accommodations. There is always access to spontaneous domestic travel and places to stay, consistent as well with past years. Portuguese fluency would not be very relevant to an itinerary volume. The Falls can be done in a shorter time (ie, 2 days) because the town is not value-added but I would not shorten an excursion to Salvador or Recife to that degree. I recall we needed an Argentine entry document to cross to the Falls’ other side. I highly recommend Pousada Guata Fora, semi-detached chalets, close to the airport and the Brazilian entrance to the park. Great breakfast and optional added buffet dinner so your nutritional needs are quickly accessible without travel into town and allows more time to enjoy the grounds. The venue also facilitated taxi transfers to the Argentine entrance across the border. If your 3 candidates do not pan out I suggest a stopover by bus to or from SP-Rio, in Ubatuba or Paraty, for an appealing small town coastal sightseeing experience. They are not on the express route but can be arranged as separate travel stretches. Bus travel purchase domestically requires passport ID. Easter is April 17th and may be busier and more expensive that weekend. -
short Jan Brazil trip report
Riobard replied to babybear2's topic in Latin America Men and Destinations
After finishing several weeks in São Paulo I decided to spend a few weeks in Rio de Janeiro though I had not at all planned it. I had been toying with going to Recife, particularly since an excursion to that destination was abruptly cancelled in March 2020. The weather was certainly better in Rio and the recently overused umbrella stayed packed away. One of the most striking things was that Tues free 1st cabin booking night, of which I attended two while there, though always packed in years gone by, was almost unmanageable. Reserving a suite involved a 90-minute wait that was best spent in more remote corners far from the maddening crowd to attenuate coronavirus exposure risk, attending the event being so very counter-intuitive with case incidence peaking there. It seems to be a locked-in ritual but with diminished returns, including for providers. You can collect phone numbers. Over the few months I tested very regularly and managed to beat the odds of a pandemic index case of infection. -
I would contentedly put out 10,000 DOP for what you described, in terms of what the provider gets, but I am not sure I would have the skills and stamina for the arranging!
-
Sounds about right. #5 may be 8,000-10,000, doing it as a big favour because it’s your lucky day, and intercourse off the table … that is, not on the bed not on the sofa not on the chaise long not on the dining room table not nowhere … but likely hot! LOL Of course I may be wrong.
-
I usually get about 1,000 reais at Calforex for about 15%. Then in Brazil BMO Mastercard linked to BMO chequing. The fee seems to be fixed at BRL20 (c $5 CDN) so I withdraw 1,000 at a time, amounting to 2% service fee. I only use Santander bank because it’s the only facility where I have not banged my head against the screen. In Rio there is a branch in my staybourhood. I don’t check exchange later because I’m not going to deviate from this but when I occasionally glance at statement records it seems consistent with what I think the true exchange multipliers yield. I always carry a few hundred because some stores’ charge gadgets do not function, even occasionally at the brothels. I was at a major supermarket chain that had never rejected my card but once I had to leave a fairly full cart behind while cursing under my breath/ In São Paulo there is a well-functioning and secure-seeming indoor Santander ATM cluster on Paulista outside Consolação Metro station a hop on-off point to Lagoa. If the typical 100 and 50 bills are depleted you may see a prompt that 20 is the available denomination and in that case a large total order such as 1,000 will be rejected. Be alert to your CDN bank account daily limit and adjust the withdrawal accordingly; the favourable exchange lately has enabled a higher BRL withdrawal but that is simply based on my chequing plan.
-
The GoGo that gotgot away …
Riobard replied to Riobard's topic in Latin America Men and Destinations
I will definitely try to work it in to an upcoming visit, do a bit of reaching out to assess how it would be set up. -
… for now. Timing can be a bitch. Top of mind obsession for months based on pics and vids. Nobody a close second, though an earlier runner-up immediately responsive on social platform viz private interaction potential, but I hold out. A quick actually essentially prohibited slip behind stage with substantial cash tips for the stripper ensemble herded together, not snubbing any one in particular. No time for numbers exchange, just a thumbs up regarding reaching out on Instagram and he has seen me and along with visual has a brief interaction reference point. This all transpires in a flash. Crickets, then a few weeks too late an acknowledgment and encouraging response regarding meet-up prospects, ie, seductive emojis … & ‘be sure to connect when return’ (I am hard typing this; no PDE-5 inhibition necessary.) Will I or won’t I pursue getting this over-idealization out of my system? A big grown man young enough to be a grandson, hell, biologically conceivably great grandson. It’s not the first time and is generally edifying not ending in tears or snowflake griping. Not born yesterday and plenty of possibly easier to access talent but, you know, that niggly small head with a persistent single-track mind of its own. That dance with the dancer. [Right, I didn’t say. Asking means not knowing better.]
-
short Jan Brazil trip report
Riobard replied to babybear2's topic in Latin America Men and Destinations
Thanks. I actually put it here because it was one of the threads where an OP expressed difficulty getting a test, though as is often the case no distinction was made about type. Some readers do prefer vague, and an attempt at elaboration and clarity is deemed over-inclusive. But when I woke up I realized I would need to tax some very short attention spans by adding that cash is king at this place and credit cards are not accepted. Anybody that wants to start a topic, say, city-specific and not exclusively antigen-centric (read USA-centric or other sovereign states without obligatory NAAT as may be the case) is welcome to import the details about this resource. My sense is that nobody here generally possesses the characteristics that would predispose them to getting wound up about the risks of plagiarism. lol -
No on two counts, including the patient and accommodating combined as one of them. I was referencing having asked something of someone I don’t deem to be an asshole. In contrast, I don’t hope for or count on anything from assholes unable to be open. More specifically, only a grandiose asshole imputes that a request such as agreeableness and forbearance is requested of them by a particular other when in fact it wasn’t solicited at all; more importantly, that other doesn’t give a shit about your reactivity. De-centre, try to stretch your attention span (oh, pin dropped, there it goes), and consider trying some content revisionism because this invariant routine is long past tiresome. It could ever barely pass as droll; now it’s just troll.
-
Oh I agree I’ve barely grazed Manny’s surface, as I already suggested based on limited contact. But the only thing I really need to know is how to get a procurer to get me the guys I want. I’m not bent on getting to braid each other’s hair; my ATM didn’t matriculate from beauty school. Because I thought it would be a breeze and was riding on a sense of lip-smacking promise held out by other punters, I am left with grasping at theories that I suppose are not readily substantiated. He came across as enthusiastic and not at all distant or dismissive, but he opined that my requirements were not easily met. If it’s a deeper game than I realized, then I must have not made the correct strategic board moves. In fact, if it’s a game at all, I’m the guy whose anticipation of diminished returns, high-output low-yield negotiating, speedily douses libidinal energy. With an actual provider the chase may up-regulate desire, to a point; with a middle-man and his sample dossier, meh. I can whack off at an 8/10 level qualitatively if the 9/10 in the flesh doesn’t materialize, though the latter of course edges out in preference. I have no life commitments that make Brazil without a realtor less accessible than the Caribbean with one. Pay the house, pay the pimp, same difference. Not much delving needed into house dynamics, AFAIK not much complexity there. Just check the tab for suite add-ons that occasionally mysteriously appear.
-
short Jan Brazil trip report
Riobard replied to babybear2's topic in Latin America Men and Destinations
Laborlife Diagnosticos in Rio … not a maternity ward … laborlife.com 5-10 minute walk from Botafogo station (southwesterly) Very professional and fast, walk-in. If you are not a nickel-and-dimer is worth it for convenience. Close to half the cost of fee-for-service equivalent in Canada. Results in PTG and English, get both versions automatically. There are other options locally but Botafogo is so accessible whether travelling south from as far as Lapa or north from Ipanema, etc. RAT 2 hrs swab to email BRL180 RT-PCR 12 hours BRL300 RT-PCR 6 hours BRL450 For searchability keywords on our GG site: COVID rapid antigen test PCR