Riobard
-
Posts
4,740 -
Joined
-
Last visited
-
Days Won
19
Content Type
Profiles
Forums
Events
Everything posted by Riobard
-
-
I am currently less pessemistic about CoronaVac in Brazil. Will elaborate today or soon. I struggle to assess efficacy meaning and accuracy unless the study results are formulated using the detailed report model framework that researchers are using to apply for USA FDA EUA. So I would have to drill down, and consume mucho vodka, to try to figure out Gamalaya Institute’s vaccine product Sputnik (Sputnik 2 may be its name if I recall). Note that various Brazilian states and municipalities are going rogue while Anvisa (their FDA equivalent) is holding firm on its standards. Since their last approval of 4-5(?) candidates for Phase 3 trials provided up until last summer, not one candidate has been authorized for study. The only one approved for efficacy research since last August was just greenlit: Quebec and Durham NC’s Medicago protein subunit type with GlaxoSmithKline’s adjuvant. There are also many other wheeling and dealings among politicians, science institutes, and third-party national and/or foreign companies behind the scenes in Brazil. I am not about to try to call an outdoor steeplechase race, in an electrical storm, with a few Zola Budds but no Usain Bolt among the competitors. (Sorry Zola, if it weren’t for that pesky South Africa variant ...)
-
I’ll have a look, but it’s labour-intensive. The way it shows up I cannot figure out who wrote it. Is S. Fry the author?
-
Semantics ... Florida Rob means SP is the only city where he went to regular sauna venues, in case reader is confused about the intrinsic contradiction. LOL Meio Mundo is New Meio Mundo and the address is around the corner from the previous address. Same building but different location technically.
-
I don’t grasp why there are two places to start topics on Latin American Men & Destinations. It seems that posters randomly select either the first one in order of display(ie, the one at the top with currently 67 posts), or the longer section below it, to start new topics and readers must look in two places for what is new. Are they not both member-only? Apologies if a rationale was provided earlier and I missed it. [I am trying again to put my question where I intended ... it worked. But why a sub-forum that is not thematically distinct from the overall section category?]
-
Furthermore, I just started this topic in the heading at the top that designated ‘member only’, but it landed down here below the pinned topics! What gives? [I got it into the intended location on the second try. But you can see the dilemma. In which of the two sections is a new topic supposed to be entered?]
-
I don’t grasp why there are two places to start topics on Latin American Men & Destinations. It seems that posters randomly select either the first one in order of display (ie, the one at the top with currently 67 posts), or the longer section below it, to start new topics and readers must look in two places for what is new. Are they not both member-only? Apologies if a rationale was provided earlier and I missed it.
-
-
Deleted, because I added a paragraph but had inadvertently first clicked quote by mistake. See the quote in the next post for the intended content.
-
Hah ... “V” is taken: vampire blood. I have dibs on Eric Northman’s.
-
No, but the song is The Grill From Ipabema.
-
Was this ‘musicale’ guy auditioning for Ídolo Brasileiro? If so, I hope nobody tips him off that he doesn’t have to blow all the judges in order to compete. ;>D
-
We need a term for it. I nominate: to coviddle ... they ended up coviddling and cuddling all the night long ... in one’s app: coviddlers welcome ... they took their pre-exposure prophylaxis for barebacking but could not bear being other than pre-vaxxed and exposed for their coviddle-fest.
-
... by “in his state” I meant geographically in the USA. The site domain registration was renewed to 03/24/2022 and did not crash, but other host/server details likely need to be worked out.
-
Sorry, most anime characters look Caucasian to me. I checked the many Lagoa dancer pictures I have but no sign of him. Black and Asian men tend to be quite underrepresented in the gogo/stripper ranks, Gabriel being one of the exceptions with whom I am personally acquainted. But I put out an inquiry to one of the drag MCs who might be recognizable to some here ...

-
Thanks for trying. That’s not it. I had not enabled Twitter account notifications in my iOS settings. I knew when I was writing my post that using the word ‘notification’ would be a problem. I will probably have to click on the ‘not interested’ each time and hope that Twitter’s brain eventually recognizes I don’t want the clutter in my timeline.
-
A gossip rag ‘ferveção’ , but it is a bit behind the times and does not provide any images of additional guys beyond those I provided. So if your Lagoa stripper isn’t depicted? ... out of luck. As I indicated, the list is not comprehensive. @davet, if you narrow the timeline better I may be able to find him, and/or if a few more physical details. There are a few fellows with Asian admixture. And did you know for certain Japanese or are you inferring it? Indigenous features are sometimes conflated with Asian/Pacific.
-
I don’t tend to get caught up in absolute financial amounts, but the dynamics of transactions are a different matter. Is charging north of 100 reais for a mere 11 Onlyfans posts a clue?
-
Stretched out ‘in paid’ is more like real life. lol ... if you edit it, my comment will go over heads.
-
I think after 7 days on Phuket, visitors can pass through the island’s ‘sealed routes’ and travel to any of the other 5 authorized provinces in the proposal, as they will have been deemed to have traditional quarantine equivalency. However, why not the run of the country? ... that was stipulated 3 weeks ago predicated on vaccination plus negative viral test then 7-days quarantine. Perhaps it is an attempt to herd tourists more systematically, but what a lot of effort to seal off the respective continent regions. Finer details to be ironed out among NCCD, CESA, CCSA, TAT, cabinet, and Phuket. Will the island residents, notwithstanding economic ruin, want to be an isolated subgroup accepting mass inoculation? Depends on attitudes. Death of a Thai man just reported due to aneurism, not related to his CoV vaccination, not helping. I agree with @tm_nycthat one of the biggest questions is vaccination dates. Ambiguous. Furthermore, it appears that uptake of CoronaVac would be the 2nd quarter vaccination predominant playbook for Phuket. In contrast, AstraZeneca is back on the table there, to be manufactured in the country and massively distributed beginning 3rd quarter. IMHO, hamburger for a regional test-case minority, rib-eye for the rest. I would rather they stream the AZ limited interim supply to Phuket. Or at the very least, a randomized longitudinal Phuket cohort comparison of the 2 products.
-
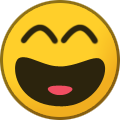
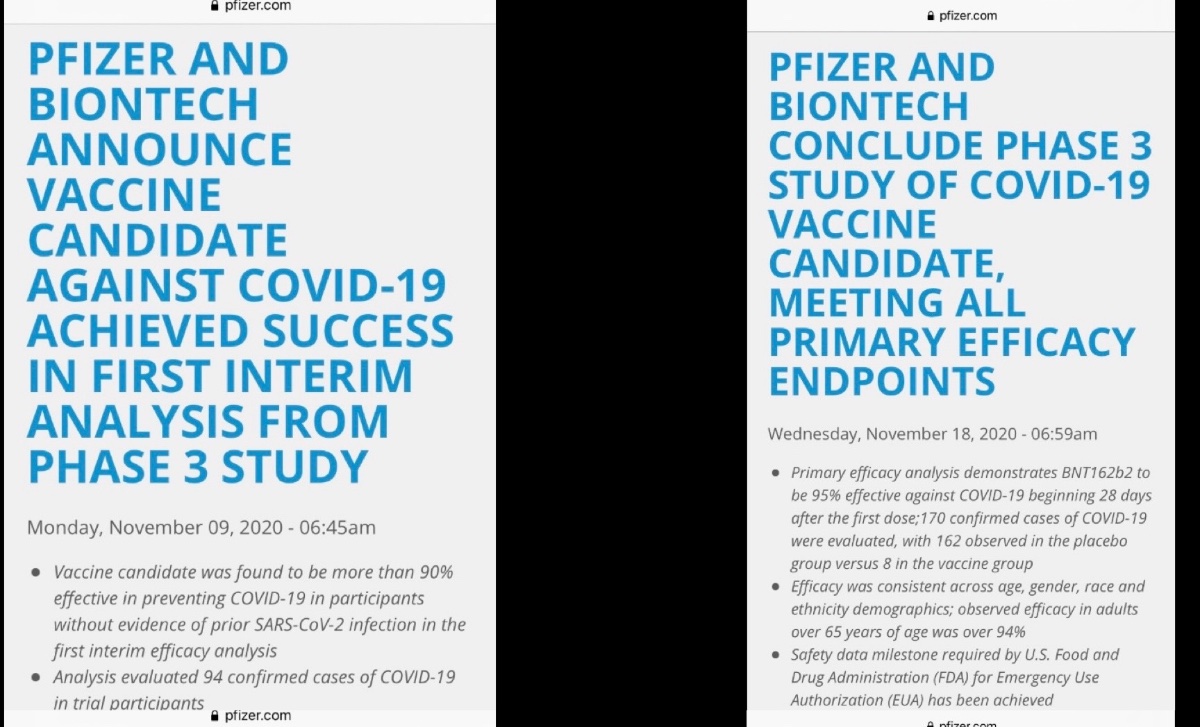
Fauci himself is an “unforced error”. My shoulder is embedded in a cold chain freezer when it comes to him and other silly pundits of his ilk. A lot of this fails the ‘conflict of interest’ smell test. The haters were willing to exacerbate vaccine hesitancy by needlessly going for AstraZeneca’s state as chum in the water. So nauseatingly egotistical and self-serving ... they are the own-goal fiasco. What the media and NIAID conveniently overlooked and neglected to mention: Pfizer/BioNTech did exactly the same thing and were, in contrast to AstraZeneca, applauded at the time. They had ‘dropped’ BNT’s hit interim efficacy and safety analysis, a week later revising it to preliminary primary analysis (stretching out taking the stock positions for a ride?). Did they already know the second press release would elevate further the positivity of the first one? Good question. The cut-off extension duration for revised analysis was oodles greater than the few days between press releases. AZ simply wanted to present its safety analysis as it was taking a drubbing based on spurious reports of embolism risk. They had not applied for FDA EUA, the vaccine possesses authorization broadly globally, and it was perfectly within their rights to present the interim analysis. They held their cool and under pressure returned immediately with primary analysis data, but they have 14 cases of plausible infection under review that they have had to defer integrating because of the stink the media raised. So there are more data forthcoming. AZ gets the last laugh on the analysis because the slight reduction in total sample efficacy was more than offset by a large increase in efficacy for age65+. But now it will be harder to disabuse the general public of notions of product inferiority. Pisses me off.
-
After months with a Twitter account I am now getting, in my feed, content stating who somebody I follow follows. Annoying, because I would just have to go their page to see those contacts. But now they are annoyingly popping up randomly. I cannot stop them like for some ads that come up and you can remove and inhibit that content. I cannot figure out any settings strategy to stop the content. I know I can just not click ‘show this thread’ but is there a way to block such notifications? Some are digital media with hundreds/thousands being followed and I worry my feed will be overrun. BTW, It does not seem related to the type of content I reply to.
-
The funeral meats have not yet gone cold, but yes there is the matter of succession. I am not qualified to give an opinion but apparently in his state, without a last will & testament or even distant living relative ... probate court likely obligated to search harder for kin so many times removed than the hospital did for a decision proxy (friend) ... but the property is deemed escheat and goes to the state. So the site’s future may be at slot-machine odds.
-
Doesn’t “sealed routes” on Phuket to prevent visits to other locations answer the question about jumping off the island?
-
What did da Nile say to da Canal? “Just relax and breathe. You can take it.”