

Riobard
-
Posts
3,804 -
Joined
-
Last visited
-
Days Won
19
Content Type
Profiles
Forums
Events
Posts posted by Riobard
-
-
Error: duplicate
-
5 hours ago, Keithambrose said:
My electrician arrived this morning, took his shoes off at the door, without my saying a word!
I believe the Health & Safety Executive calls that a strip-o-gram. Is it your birthday?

- xpaulo and KeepItReal
-
 1
1
-
 1
1
-
So Todd from the Emmy-nominated series The Jury , a show with ultimate blindsiding, was really onto something, although if you have a vehicle acceptable footwear in this case could more easily be stashed. I agree it should have been a foreseeable contingency to which you had been clued in ahead of time. Seems like you bit your tongue, not a barefoot cuntessa. This is a Candadian point of view.

-
3 hours ago, Canadianbtmguy said:
I wanted to acknowledge the accuracy of the first paragraph that while both Truvada and Descovy, are approved for PrEP generally, only Truvada is approved for on-demand/2-1-1, and I did not know that.
That being said, my PrEP prescriber said it was not approved "yet" and he did not see any reason why this very similar medication would not be eventually approved; he said that if someone was going to have sex and did not have Truvada it would not be an inappropriate choice. (Grated the GP and my situation was not exactly that: the doctor's example was that someone was going to have sex regardless; ours was that he would provided that he had PrEP)
As to the third paragraph, I'm not really sure of the harm of such a revelation. To him: is there any doubt that patients regularly reveal taking drugs that are not only not-ANVISA-approval but illegal? To me: dispensing non-ANVISA approved medications without a pharmacy license? 🤣
Your intentions were good but I was just wondering what the impact on the fellow would be in terms of his views about you if a local clinician were to later reflect that the drug and dosage of his initiation was incorrect. In actuality, he might be more inclined to seek PrEP at this point and that is not a bad thing. He might not know enough to realize the medication disconnect if and when Truvada is dispensed. Anyway, as you indicate, now you know.
It’s certainly not egregious to sub one for the other in a pinch according to the idea that having some prophylaxis is better than none.
However, the prospects for eventual on-demand Descovy appear slim. There is no registered trial assessing its non-inferiority to event-driven Truvada. There is minimal interest in additional innovative on-demand regimens and the strategy of trading off specific drug toxicities in reduced uptake may be less paramount.
One proposed study has not achieved lift-off. Even if it gets off the ground the endpoint is about 2028. It is no longer feasible ethically to have placebo-control arms, so how to approximate a gold standard method is more complex. Although the Descovy comparator is Truvada, the control group idea is substituted with background HIV incidence in non-recruited MSM. That itself reduces the analytical rigour. Moreover, the methodology described is the usual Truvada 2-1-1 but Descovy 1-1 (reduced lead-in dose loading as well as absent the final post-intercourse ‘for good measure’ dose), counterintuitive relative to the logical assumption of equal number of tablets one would expect in study arms. Demonstrating daily Descovy for vaginal intercourse PrEP efficacy is probably of greater importance.
-
AFAIK Descovy, in contrast to Truvada, is not indicated anywhere for on-demand / event-driven 2-1-1 HIV PrEP either formally or off-label, as corroborated by NYC Health, IAS, CATIE, etc.
One can switch from daily or on-demand Truvada to daily (but not on-demand) Descovy, or from daily Descovy to daily or on-demand Truvada. Descovy has not been studied for oral uptake timing surrounding sexual intercourse events.
Not that I would consider giving a “starter kit” to a Brazilian national in Brazil because I would more likely steer them to their local provision option, but I would recommend accurate educational guidance. Also, unlike Truvada and Apretude, Descovy for PrEP is not yet authorized in Brazil. If the guy were to eventually seek PrEP formally he might reveal that a visiting gringo had provided a controlled prescription-dependent drug not ANVISA-approved in Brazil and with an incorrect dosing regimen instruction to boot.
- KeepItReal and floridarob
-
2
-
-
Who really wants to enter robust pushback against travel advisories, as safety cannot be guaranteed? All I can share is that my post-pandemic trip to Medellín and DIY side excursion to Guatapé was a very positive experience. Easy to get to major arts/culture venues by Metro or walking. Great food. Well-heeled locals milling about. Stays in Poblado and Estadio/Laureles in unexpectedly upscale surroundings. My only comment would be that 12 days is a bit long and in that time period I combined Medellín (gateway location) with a trip to Bogotá via Satena Air.
That said, I would personally likely prefer a European river cruise over a return to Medellín, if hires were to be out of the equation, because I prefer novelty to retracing sightseeing steps.
-
26 minutes ago, Londoner said:
… Three years ago, a friend of my boyfriend, someone whom I've known for over a decade, forty years-old, a university graduate from a middle-class family and not on the scene, was found to be positive. He was quickly medicated.
However, two years ago he was taken seriously ill with a series of ailments, one of which was life-threatening. He was in hospital for months. The doctor told him the symptoms were Hiv related. He's better now, but still suffers distressing after effects from his illness.
I've never doubted the importance of safe sex but even I was surprised by what happened to him; after all, there is a belief in some quarters that new medication makes the condition manageable, like diabetes 2. I know now that it remains life-threatening, and probably will continue to be so for many years.
Could have been IRIS, the sobering, paradoxical, not uncommon sequelae of HIV drug treatment. Surprisingly not very much on the awareness radar of higher HIV risk-taking populations even though known about for decades.
https://www.ncbi.nlm.nih.gov/books/NBK567803/#:~:text=Immune reconstitution inflammatory syndrome (IRIS,of IRIS is still unknown. -
It’s a question of lead-in dosing, depending on what is predictable and practical, for sufficient mucosal drug concentrations. On-demand or event-driven method 2-1-1 (and then daily ongoing or repeat 2-1-1 depending on activity break durations) with the double dose 2-24 hours before first sexual encounter will provide initial protective drug concentration. Alternatively, a week of daily single dose while celibate with respect to risk: essentially [1-1-1-1-1-1-1] - 1-1 …
I have greater hesitancy for the on-demand method until a few days of the single dosing are done and dusted, but use condoms for anal anyway.
The pharmacology investigators of drug concentrations based on 4 doses weekly (not to be conflated with 2-1-1) nevertheless consider daily dosing to be a more robust recommendation as that regimen has more routinization and affords drug concentrations expected to persist in the protective range in the event of missed doses.
-
1 hour ago, ausken said:
I assume the 7-Eleven checkout staff can handle the off fees and drinks for the guys? This could be a lucrative new business for 7-Eleven to get into!
Slurpers overheard: “Shall we head to 7-Eleven to off a few Slurpees?”




-
… as announced this evening by Brazil’s Ministry of Tourism and Official Gazette of the Union with a few hours to spare. The revised start date had previously been set for midnight for American, Canadian, and Australian visitors.
- Connordrick, floridarob and sydneyboy1
-
3
-
All indications are that the topic is scheduled further for government Plenary sessions, including today, although the legislative website suggests that today’s planned Plenary is not being held after all. Nothing is certain come Wednesday.
-
Back to Brazil following the Venezuela excursion.
All over the news is the requirement for the visa commencing April 10th. It appears to be on after all. The discourse continues to be tension between reciprocity and tourism wellness.
It seems that the one-year postponement agreement was a bluff, a stall, and has not been ratified. Apparently a vote to revoke can still go forward but time is running out.
-
7 hours ago, Hunkz said:
According to this site the Brazilian government will drop the upcoming visa requirements for Americans, Canadians, and Australians https://brazilian.report/liveblog/politics-insider/2024/03/28/lula-to-drop-visa-requirements-us-citizens/. Not sure how trustworthy they are but hopefully it turns out to be true.
Actually, according to several news sources there is a distinct possibility that the requirement will be postponed to April 10th, 2025 as opposed to entirely revoked, supposedly a concession made to circumvent an immediate vote to scrap it or maintain it, immediate defeat for one or the other side of the issue. I think it could play out for a few more weeks.
-
Some bakeshops offer it.

-
No placebo control group or crossover treatment-placebo arms for either Futura study on which the efficacy and authorization is assessed. The comparator study indicated oral tadalafil 5 mg (lowest dose) worked better.
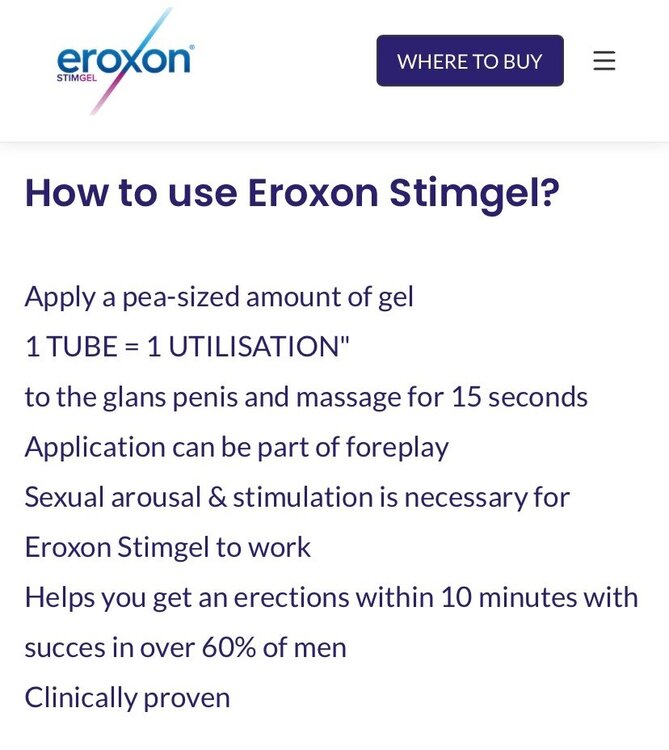
Endpoint of sustained erection for intercourse: 47% of subjects that did not meet this goal at baseline reported achieving it at follow-up. Outcome of erection sufficient for penetration was a little better; 64% that could not at baseline could achieve this at follow-up.
The premise is evaporative action, cooling then warming effect that apparently increases the smooth muscle relaxant nitric oxide; effective local levels of nitric oxide need to be achieved. It is unlikely that applying the gel alone would do much; it must be combined with the usual measures that promote arousal. What is unknown about public domain reviews is whether some consumers apply the product without concomitant sexualizing.
That said, I am skeptical about Eroxon. It seems to me that after a brief time any temperature effect would wear off and any initial additional burst of nitric oxide and blood flow would be shortlived.
- dscrtsldnbi and unicorn
-
2
-
Technically it’s not medicine, medication, or a drug. It is classified as a medical device, the bar set lower for authorization.
-
If you want to impress me as a company you need to decide whether it is success or sucks, and spell correctly.
-
-
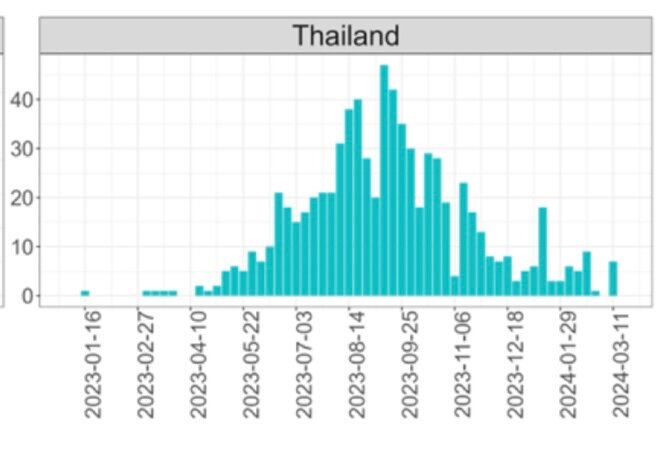
The Mpox vaccination question:
Still predominantly MSM age 18-39 infection case susceptibility, but WHO’s epidemiological tracking for Thailand indicates that from November to mid-March the new case incidence for the country averaged merely about one per day, consistent downward trend from last August.
- vinapu, KeepItReal and khaolakguy
-
1
-
 2
2
-
Draden’s 3rd question posed above:
My observations on Airbnb:
Where possible, I often take Airbnb lodgings particularly for longer trips. This winter I booked 30 nights in a large one-bedroom apartment. It was decent, well-managed, excellent location easily walkable to the Silom/Surawong area action. I also took a nice hotel room for the trip for entertaining without any valuable belongings to worry about, with bottomless towel supply options, and without dealing with the impossibility of sleeping with the usual paper-thin walls and constant inconsiderate slamming of doors that typically occurs in hotels.
There would not have been a problem bringing guests, within reason, to the Airbnb condo. My “trainer” came up a few times. I don’t do overnights with guests.
I was to check in on the 4th day as I technically needed 27 nights but I aligned with the one-month guideline. There is a lengthy thread here from around March 2023 on this subject.
The “Superhosts” objected to the add-on because they thought it was unfair and unnecessary. Their point was that it’s up to me but they preferred to not take the extra fee needlessly. I had raised my concerns regarding lodgings regulations and they proclaimed that they were not operating outside of guidelines. Most of the many stellar reviews appeared to be short period stays. They capitulated to my insistence.
There were no hassles whatsoever. Key pickup was from the reception staff and there was no prohibitive sign anywhere. I needed a few minor items for the kitchen and the hosts ordered them online and communicated with reception for delivery and pickup. Reception clearly knew I was a farang. I had even printed off the contract in case airport immigration were to have grilled me but it was stamp-and-go.
The building had a few shops in the lobby. Other buildings in the area were similarly structured with mini-malls and some had Airbnb logo signs prominently displayed.
In October the national Hotel Act regulations were revised. A lot of dwellings qualify for hotel licensing exemption and hosts can apply formally using an online form. The room threshold was lifted from 4 to 8. The examples include villas, tents, rafts, and shipping containers. (Note that shipping containers were part of Qatar’s World Cup accommodations options). Condo apartments are neither listed as an example nor excluded. Clearly the aim is greater flexibility.
Some cities globally require that hosts must reside in the unit as a principal residence and only let their unit when they are willing and able to vacate it. Such a stipulation does not exist in Thailand.
My sense is that condominium directorship boards can nevertheless trump the above workaround and behave as a separate entity to restrict short-term rentals. My advice, then, is to clarify with an Airbnb host that they are not operating under the radar … that they have formally sought and obtained permission for the hotel license exemption, that the building has not imposed restrictions, and that they are operating within any requirements regarding lodgings inspection, income subject to tax, VAT obligations, etc.
-
-
-
1 hour ago, geodesic said:
The link you posted seems to be down, Riobard.
Do you think the place is worth a visit?
It opens for me. It’s an Instagram page so you must have Instagram activated.
I have not been in spite of ample opportunity. It does not particularly resonate with me as worth the additional effort. I prefer a more sure thing. I am also more likely to take a side trip to a different city and blend sightseeing with exploring trade venues that might be on offer.





Is "Intimacy Director" a new job?
in The Beer Bar
Posted
If you think it’s a novel gig in general then you haven’t been following half of the post content on this board.😉